Download to read offline

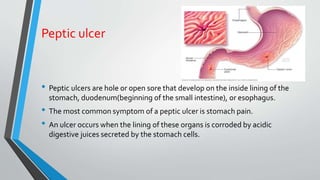



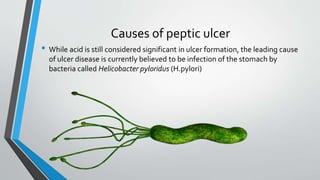










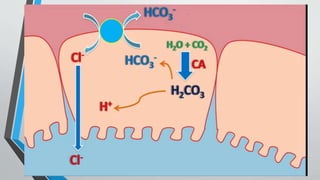






















































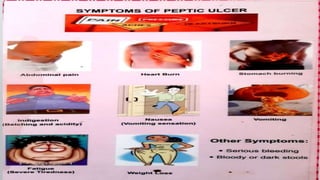




Peptic ulcers develop in the lining of the stomach, duodenum, or esophagus when acidic digestive juices damage the protective mucus layer. Common symptoms include stomach pain relieved by food or antacids. While acid contributes to ulcer formation, infection with H. pylori bacteria is now the leading cause. Treatment focuses on reducing acid with H2 blockers or proton pump inhibitors, eliminating H. pylori, and counseling lifestyle changes.



































































