Download to read offline
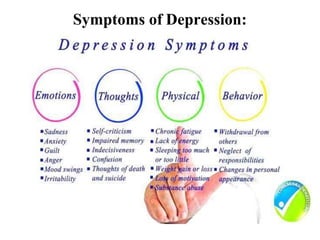
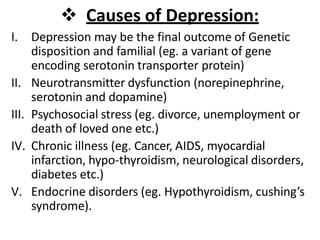
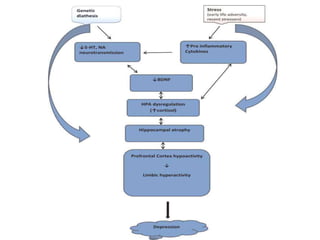
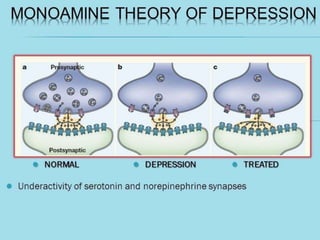
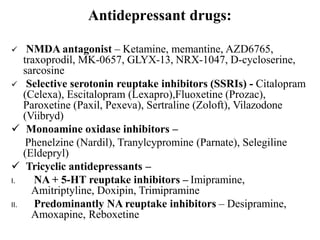
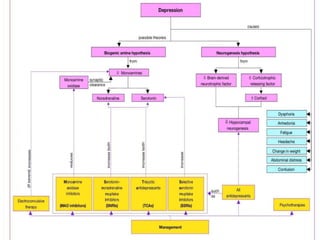
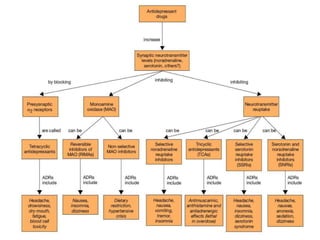

Depression is a state of low mood and lack of interest that affects thoughts, behavior, feelings, and well-being. It has various causes such as genetics, neurotransmitter dysfunction, psychosocial stress, medical illnesses, and endocrine disorders. There are two main types of depression: unipolar, which accounts for 80% of cases, and bipolar disorder. Treatment involves antidepressant drugs which affect serotonin, norepinephrine, and dopamine levels, as well as electroconvulsive therapy for severe cases. The pathophysiology involves both neurotrophic and monoamine hypotheses relating to brain-derived neurotrophic factor levels and deficiencies in cortical monoamines.






















































































