Download as PDF, PPTX


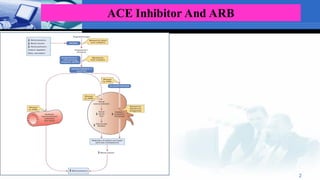
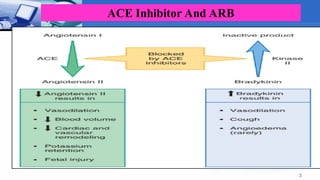
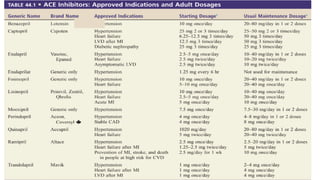
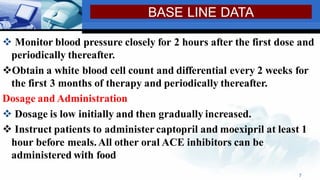
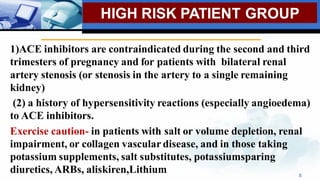
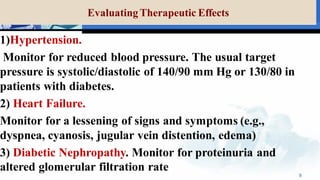
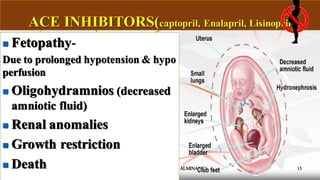

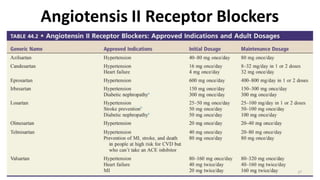


ACE inhibitors and ARBs are commonly used to treat hypertension and heart failure. Some key points about their use include: - ACE inhibitors work by inhibiting angiotensin-converting enzyme, while ARBs block the angiotensin II receptor. Both lower blood pressure. - High-risk groups for ACE inhibitors and ARBs include those with renal artery stenosis or who are pregnant. Close monitoring of blood pressure and potassium is needed. - Adverse effects include cough, angioedema, hyperkalemia, and fetal injury if taken during pregnancy. Drug interactions can intensify effects, so concomitant NSAID or potassium supplement use requires caution. - Proper dosing and






















































































