1) Structural defects of teeth can range from minor issues like pitting or discoloration to more serious problems caused by genetic factors, metabolic diseases, or infections during development.
2) Common defects include amelogenesis imperfecta, which affects enamel formation due to genetic mutations; and dentinogenesis imperfecta, where defects in collagen result in soft, translucent teeth with bulbous crowns and short roots.
3) Other defects include molar incisor hypomineralization from systemic factors during development; regional odontodysplasia, a localized disorder affecting a group of teeth; and rarer conditions like dentinal dysplasia. Treatment depends on the specific defect but aims to
Introduction
• Structural defectsof teeth may be minor (Pitting or Discoloration) or
serious
• They may be markers of past disease – rarely still active
• Their etiology may be genetic, metabolic or infection
• They may result from defects in calcification, formation of collagen
matrix or incorporation of a substance into the enamel resulting in
discoloration
• May lead to compromise in the strength of teeth or just pose a
cosmetic challenge
• Treatment may range from crowning to mare cosmetic improvement
in order to improve aesthetics
3.
DEFECTS OF DECIDUOUSTEETH
• These are rare – because calcification of teeth occurs in the fourth
month of intrauterine life and disturbances of metabolism and
infection occurring at that stage often leads to abortions
• They often constitute discoloration due to
I. Excessively high water fluoride – mottling
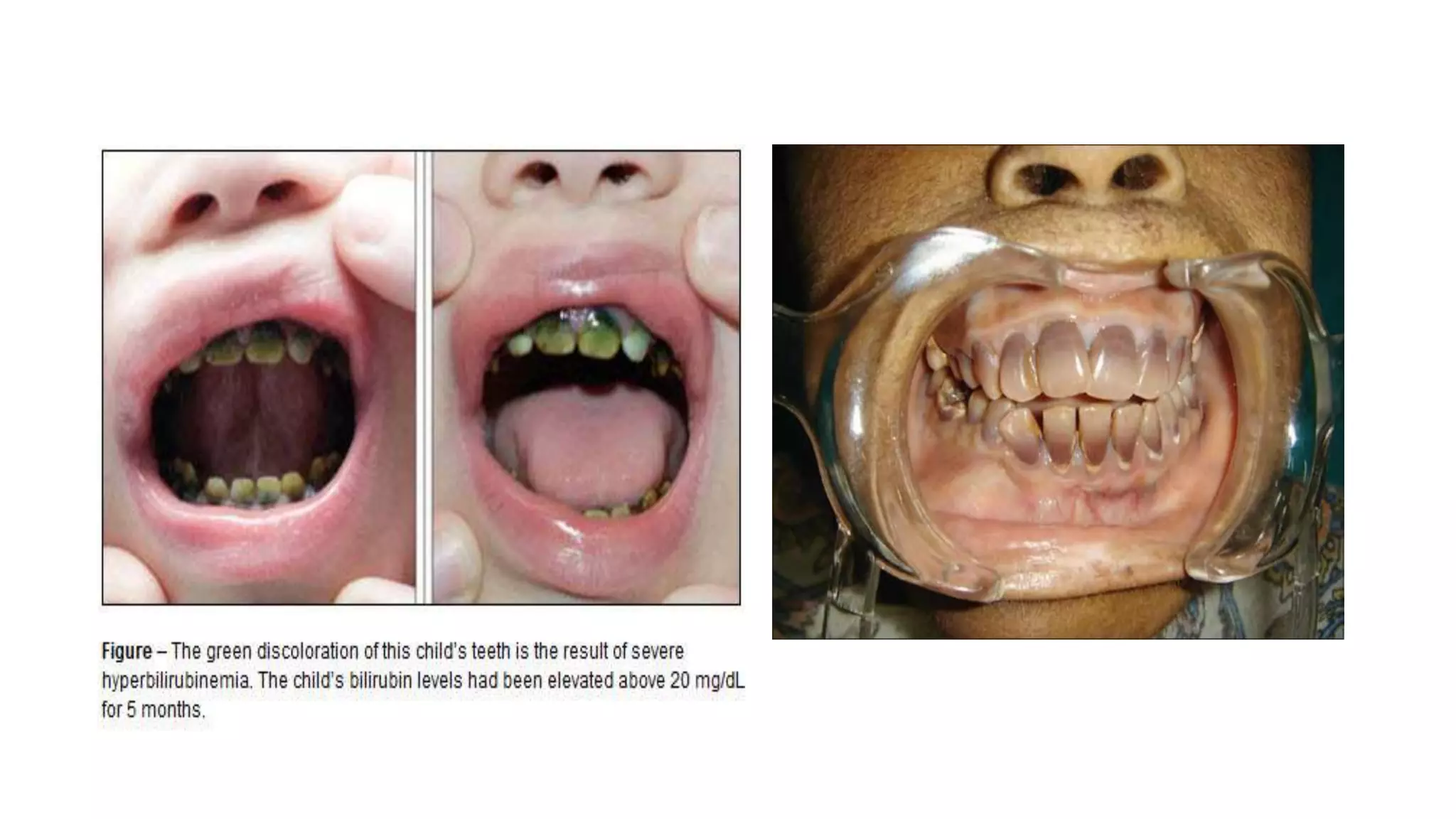
II. Abnormal pigments in the body due to
Neonatal Jaundice – yellow teeth or bands of greenish
discoloration
Congenital porphyria – teeth are red or purple
Tetracycline
DEFECTS OF PERMANENTTEETH
Permanent teeth defects may involve
I. Single tooth - Local causes such as periapical infection of predecessor tooth
II. Multiple teeth – due to systemic diseases
o Among these defects due to systemic causes are Amelogenesis imperfecta and
Dentinogenesis imperfecta
Amelogenesis Imperfecta
This is a group of conditions caused by defects in the genes encoding enamel matrix
proteins
It is a genetic disorder whose pattern of inheritance can be
I. Autosomal dominant or recessive - most common and caused by mutations
in the AMEL X gene which codes for Ameloblastin, Enamelin or tuftelin
II. X-linked – less common and results from defects in amelogenin genes
7.
Because the defectis due genetic factors, all the teeth are
affected and defects involve the whole or randomly
distributed in the enamel
This is in contrast to defects seen due to exogenous causes
that only act for a brief period and so cause defects related
to that period of enamel formation
The exception in flourosis
Amelogenesis imperfecta can be classified as
I. Hypoplastic
II. Hypomaturation
III. Hypocalcified
8.
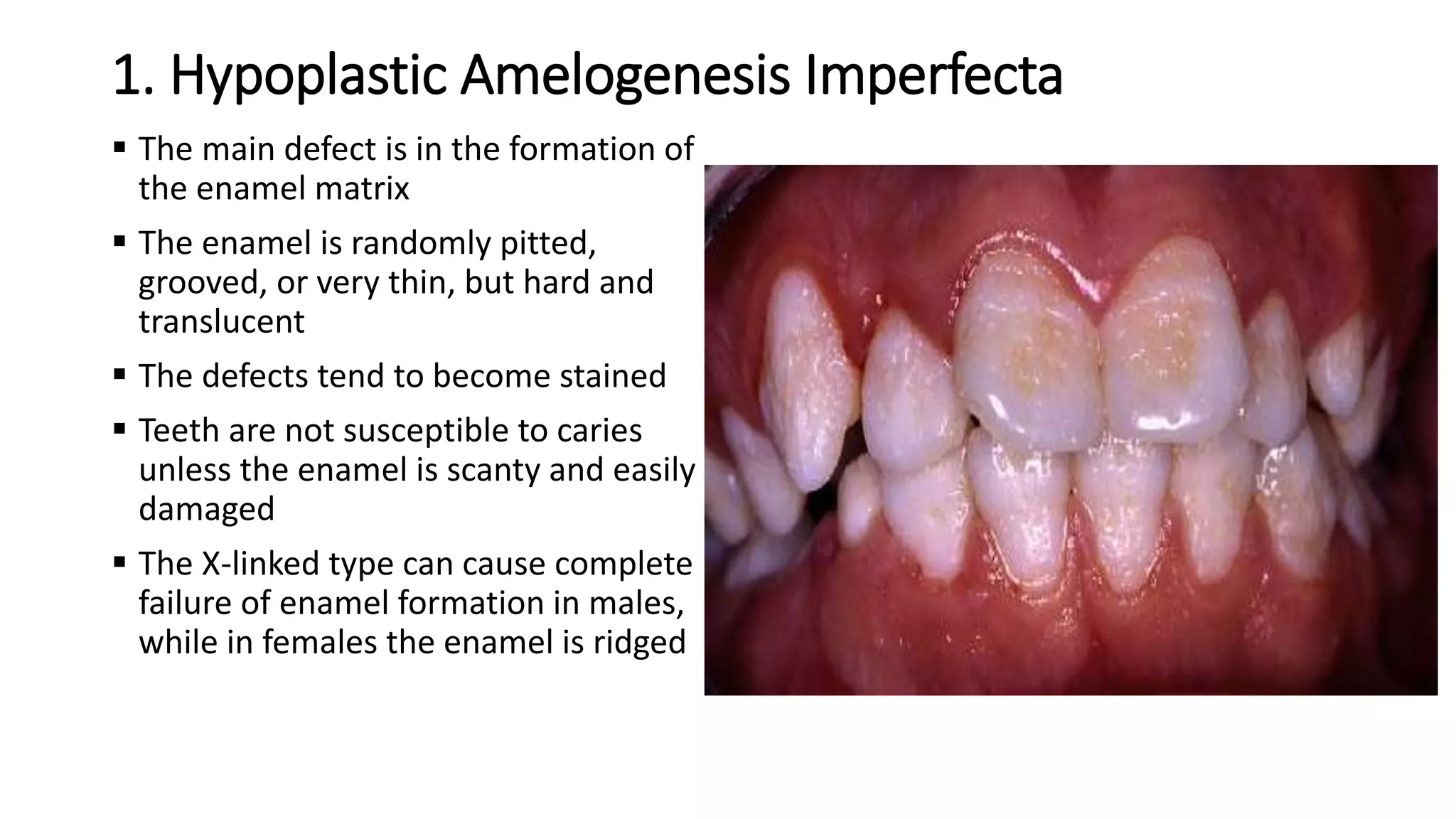
1. Hypoplastic AmelogenesisImperfecta
The main defect is in the formation of
the enamel matrix
The enamel is randomly pitted,
grooved, or very thin, but hard and
translucent
The defects tend to become stained
Teeth are not susceptible to caries
unless the enamel is scanty and easily
damaged
The X-linked type can cause complete
failure of enamel formation in males,
while in females the enamel is ridged
9.
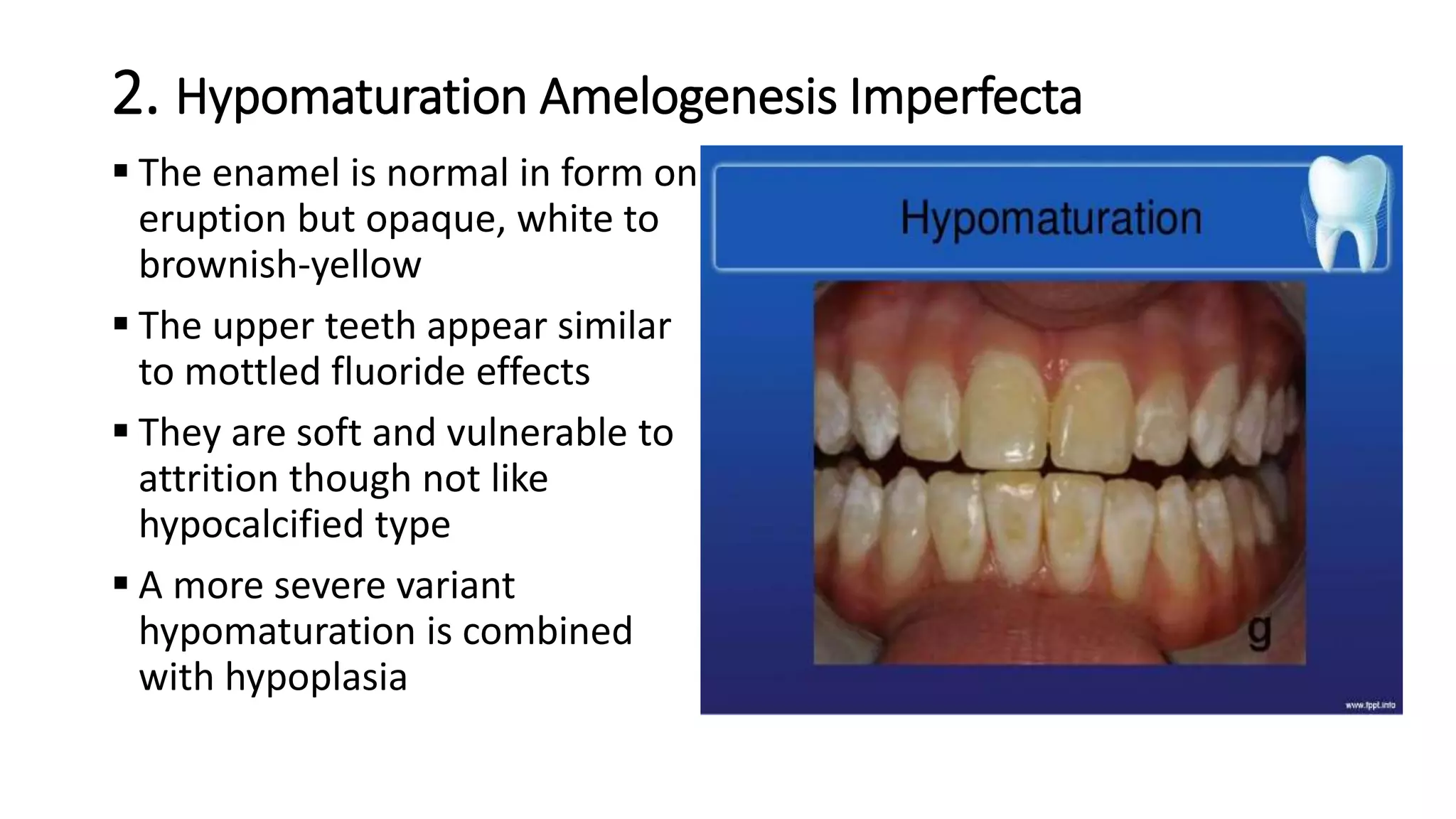
2. Hypomaturation AmelogenesisImperfecta
The enamel is normal in form on
eruption but opaque, white to
brownish-yellow
The upper teeth appear similar
to mottled fluoride effects
They are soft and vulnerable to
attrition though not like
hypocalcified type
A more severe variant
hypomaturation is combined
with hypoplasia
10.
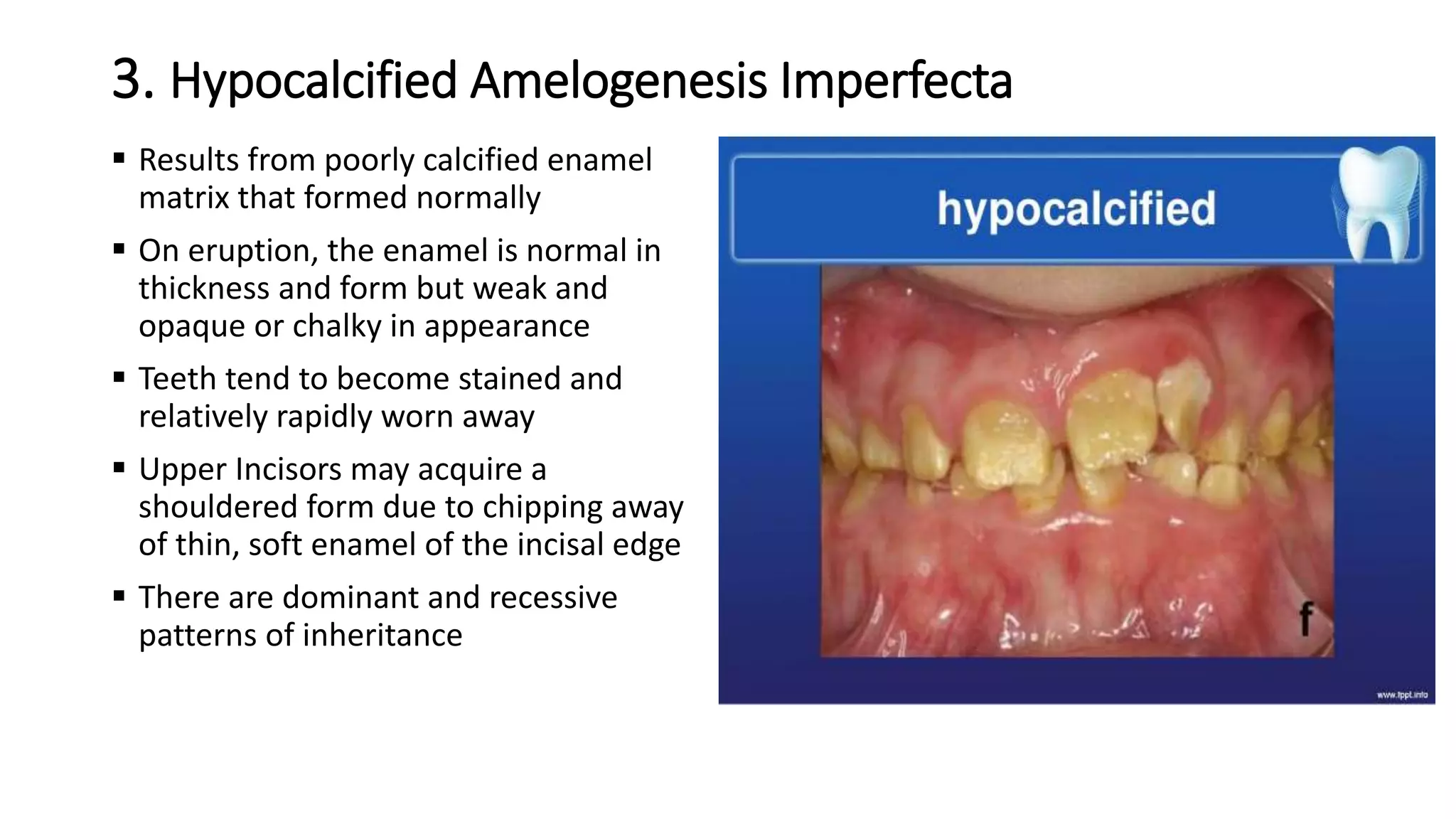
3. Hypocalcified AmelogenesisImperfecta
Results from poorly calcified enamel
matrix that formed normally
On eruption, the enamel is normal in
thickness and form but weak and
opaque or chalky in appearance
Teeth tend to become stained and
relatively rapidly worn away
Upper Incisors may acquire a
shouldered form due to chipping away
of thin, soft enamel of the incisal edge
There are dominant and recessive
patterns of inheritance
11.
Molar Incisor Hypomineralization(MIH)
This is defined as hypomineralization of variable severity associated with
systemic factors and affecting one or more permanent first molars with or
without incisors involvement
The etiology is unknown but is thought to be associated with many of the
factors described above including infections of upper aerodigestive tract,
fevers and antibiotics
It presents as well delineated white, yellow or brown opacities usually on
the buccal or occlusal surfaces
Involved teeth are prone to thermal sensitivity and caries
Management includes early diagnosis, remineralization, caries prevention,
restorations
12.
DENTINOGENESIS (ODONTOGENESIS) IMPERFECTA
This defect is uncommon. It is due to defects in collagen formation
It is transmitted as an autosomal dominant trait
The defective gene is closely related to osteogenesis imperfecta
In types III and IV osteogenesis imperfecta, dentinogenesis imperfecta is
present in over 80% in the primary dentition
Tooth discoloration and attrition are less severe in permanent teeth
Class III malocclusion is associated in over 70%
In type III disease, dental development is delayed in 20% but in type IV disease
it is accelerated in over 20%
The dentine is soft and has an abnormally high water content
13.
Clinical Features
Enamelappears normal but uniformly brownish or purplish and
abnormally translucent
Teeth form is normal but crowns of molars are bulbous and roots are
short
Enamel is weakly attached and tends to easily chip away from dentine
Teeth can easily be worn away down to the gingivae in severe cases
necessitating early fitting of full dentures
Only a few teeth may be involved in some patients, while others
remain normal
Radiographically, the main features are obliterated pulp chamber and
stunted roots
14.
Pathology
The earliest formeddentine at ADJ usually appears normal
Deeper tissue is more defective: tubules become few,
calcification is incomplete and the matrix is imperfectly
formed
The pulp chamber becomes obliterated early and
odontoblasts degenerate
Scalloping of the ADJ is sometimes absent
The enamel tends to split away from the dentine but is
otherwise normal in typical cases
15.
Shell Teeth (Dentinogenesis Imperfecta Type 3)
In this type, only a thin shell of hard dental tissue surrounds overlarge pulp
chambers
There is normal but thin mantle dentine that covers irregular dentine
The pulp lacks a normal ondotogenic layer and consists of coarse connective
tissue which becomes incorporated into the deep surface of the dentine
Dentinal Dysplasia ( Rootless Teeth)
In this condition, the roots are very short and conical
Pulp chambers are obliterated by multiple nodules of poorly
organised dentine
Affected teeth tend to be lost early in life
16.
REGIONAL ODONTODYSPLASIA (GHOSTTEETH)
This is a localized disorder of development affecting a group of teeth in
which there severe abnormalities of enamel, dentine and pulp
Its aetiology is unknown though a few cases have been associated with
facial vascular naevi or abnormalities such as hydrocephalus
Clinical Features
Regional odontodysplasia – recognisable at time eruption
Maxillary teeth are most affected
Affects either one or both dentitions and involves one or, at most, two quadrants
Involved teeth may fail to erupt but if they do, show yellowish deformed crowns
with a rough surface
Affected teeth have an enlarged pulp chamber surrounded by thin enamel and
dentine
17.
Cont..
Radiographically, theteeth appear crumpled and abnormally radiolucent or
hazy due to the paucity of dental hard tissues – hence ‘ghost teeth’
Histologically,
the enamel thickness is highly irregular and lacks a well-defined prismatic
structure.
The dentine has a disordered tubular system and contains clefts and
interglobular dentine mixed with amorphous tissue
The surrounding follicle tissue may contain small calcifications
If they erupt, the involved teeth are susceptible to caries and fractures and
their complications.
They can be restored and so preserved to allow dentine formation to continue