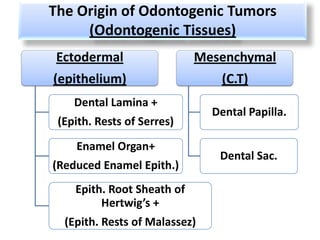
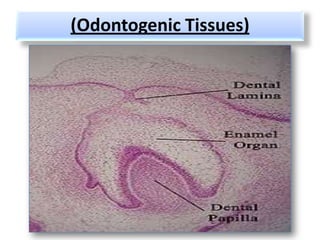
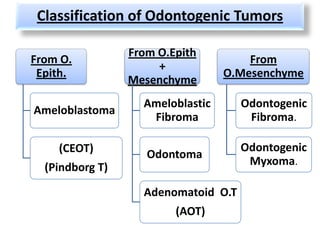
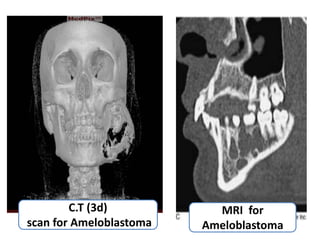
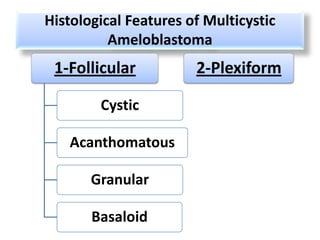
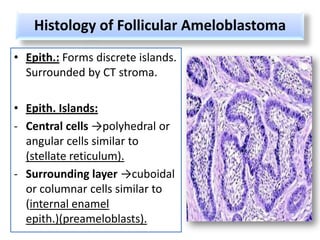
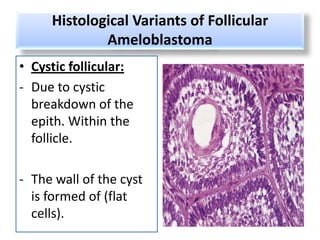
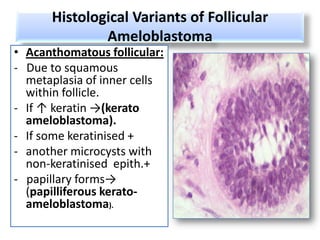
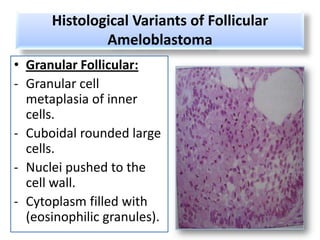
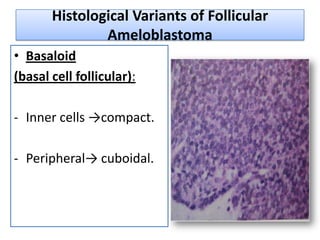
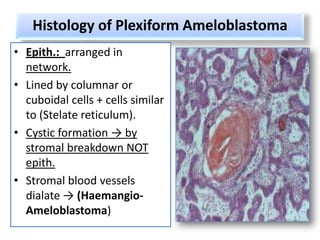
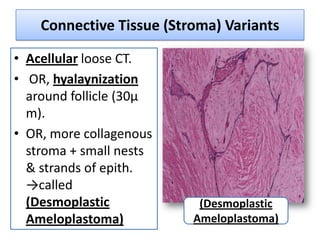
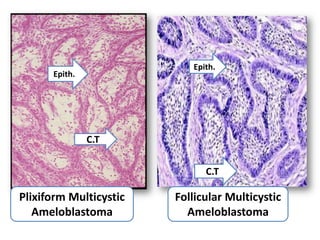
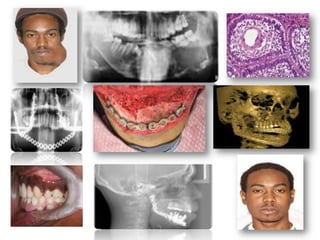
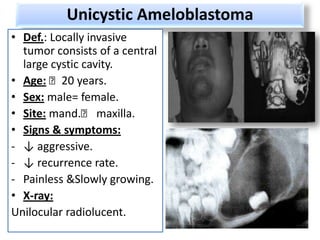

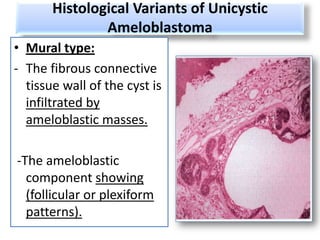
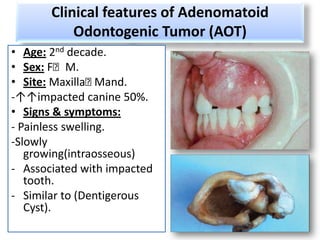
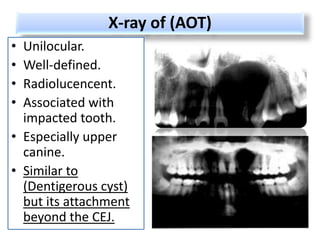
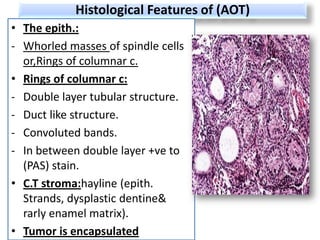
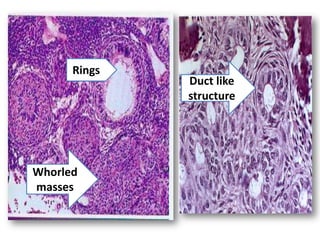
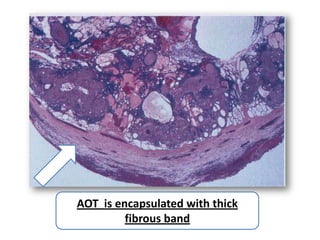
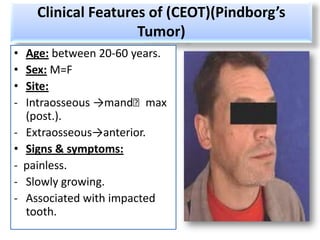
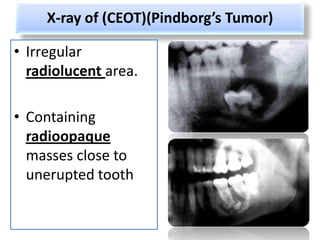
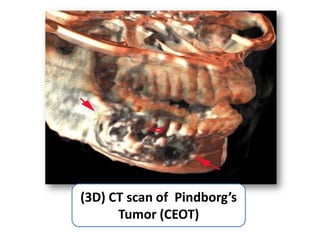
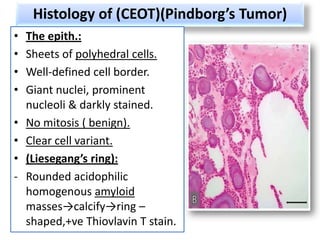
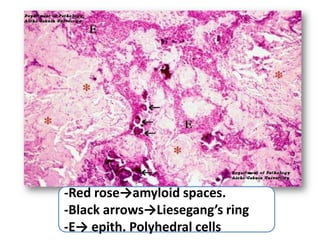
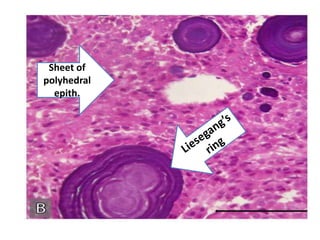
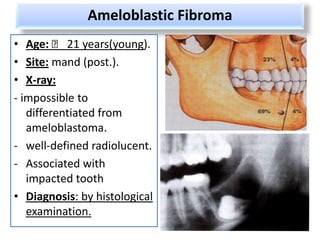
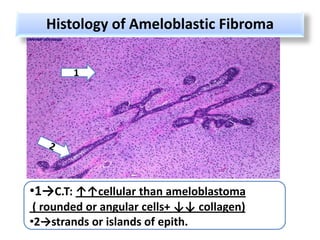
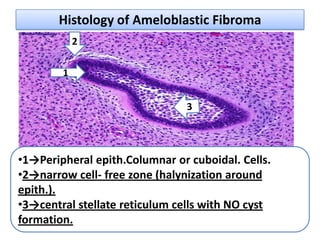
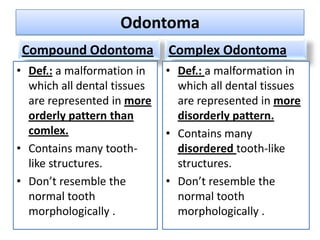
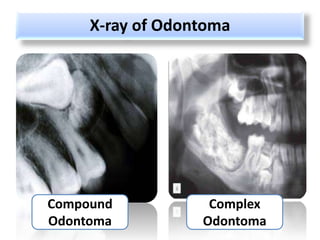
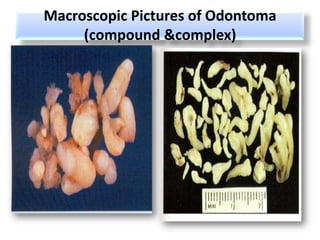
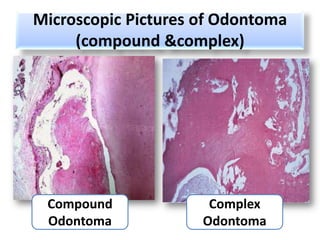
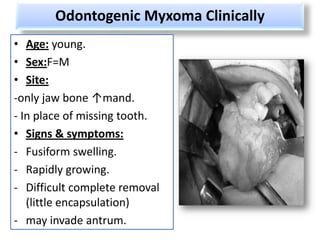
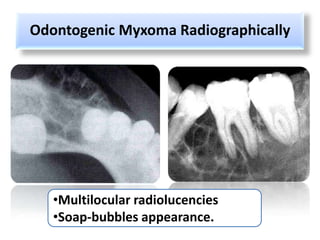
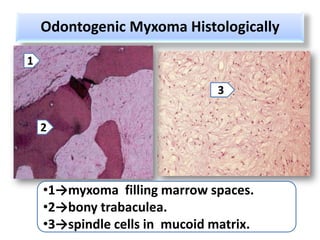

This document defines and describes odontogenic tumors, which are neoplasms or tumor-like malformations arising from odontogenic tissues. It classifies various odontogenic tumors based on their origin from odontogenic epithelium, mesenchyme, or mixed tissues. Key tumors discussed include ameloblastoma, adenomatoid odontogenic tumor (AOT), calcifying epithelial odontogenic tumor (CEOT), and ameloblastic fibroma. Clinical features, imaging findings, and histopathological characteristics are provided for each tumor type.














































































