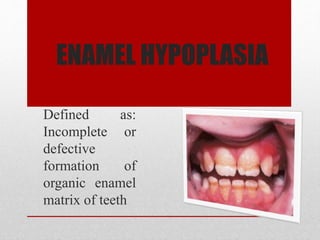
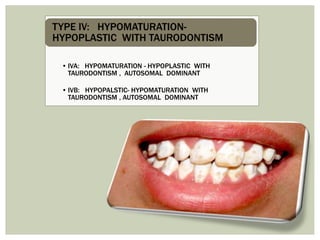
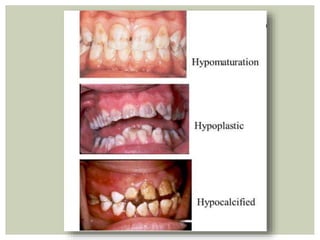
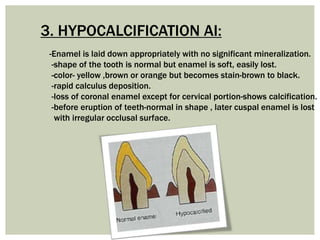
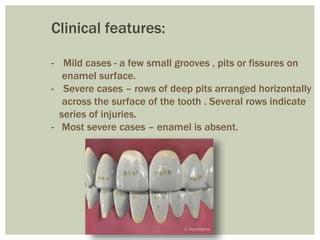
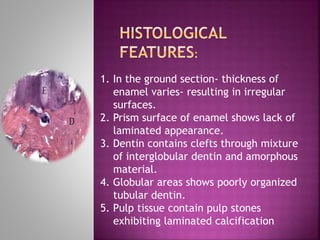
This document summarizes structural anomalies of teeth, focusing on enamel hypoplasia. It describes the causes of enamel hypoplasia including nutritional deficiencies, infections, trauma, and fluoride ingestion. The key types of enamel hypoplasia are discussed - hypoplastic, hypocalcified, and hypomaturation. Clinical features and classifications of amelogenesis imperfecta are provided for each type. Histopathological features and treatments are also briefly mentioned.