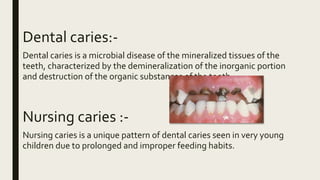
Nursing bottle caries is a pattern of early childhood dental decay seen in young children due to prolonged and improper feeding habits like unrestricted bottle feeding. It is caused by fermentable carbohydrates like milk, fruit juice and honey interacting with the bacteria Streptococcus mutans in the mouth over long periods without saliva flow to wash them away, such as during sleep with a bottle. This leads to acid production and demineralization of tooth enamel. Management involves treating decay, counseling parents on proper feeding and oral hygiene, and preventing recurrence through dietary control and fluoride therapy. Complications can include pain, malocclusion and speech problems if left untreated.