Downloaded 296 times
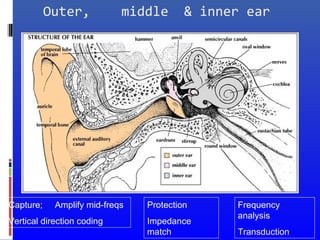
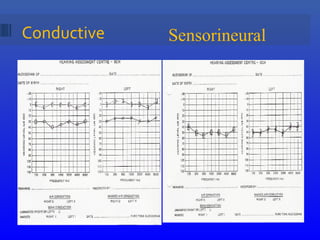






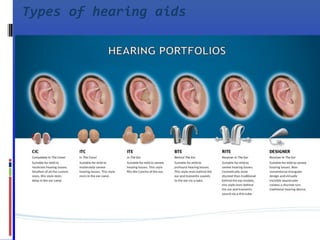
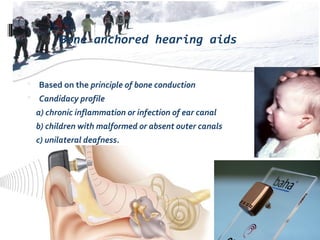
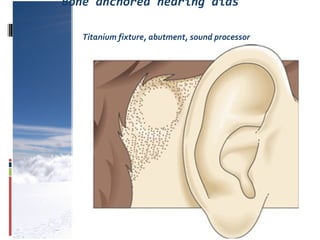
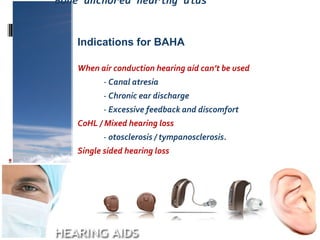

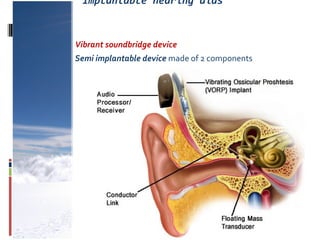
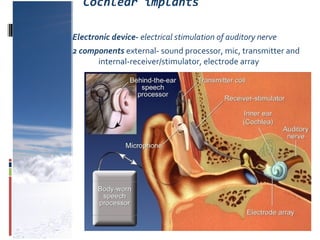
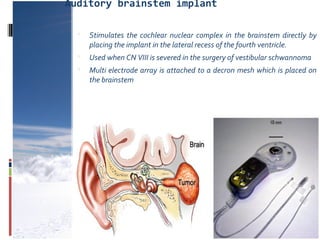
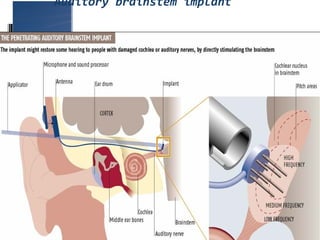





This document discusses deafness and hearing loss. It defines different types and degrees of hearing loss. Conductive hearing loss occurs when sound is not conducted properly through the outer or middle ear. Sensorineural hearing loss occurs due to damage to the inner ear or auditory nerve. Mixed hearing loss has both conductive and sensorineural components. Rehabilitation methods are described including hearing aids, bone anchored hearing aids, cochlear implants, and auditory brainstem implants. Types of hearing aids and how they work are explained. Speech reading, auditory training, and education of the deaf are important rehabilitation strategies. The overall message is that untreated hearing loss is more noticeable than using hearing aids or other assistive devices.























































































