Downloaded 1,204 times


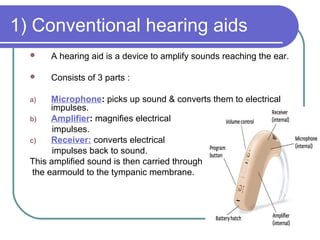








































Hearing aids and implantable devices can help people with hearing loss. Conventional hearing aids consist of a microphone, amplifier and receiver. They come in different styles like behind-the-ear or in-the-ear. Bone anchored hearing aids use bone conduction to bypass the outer/middle ear. Cochlear implants have an internal and external component and provide electrical stimulation of the auditory nerve for severe-profound loss. Implantable hearing aids use direct mechanical vibration of the ossicles. Candidates for these devices have moderate-severe loss and limited benefit from conventional aids.






























































![cochlear implant [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cochlearimplantautosaved-230807191245-e9fc2957-thumbnail.jpg?width=640&height=640&fit=bounds)
























