Downloaded 31 times

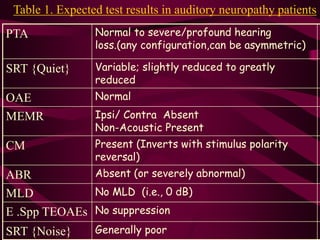
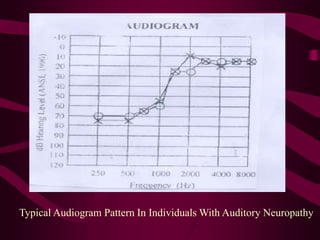
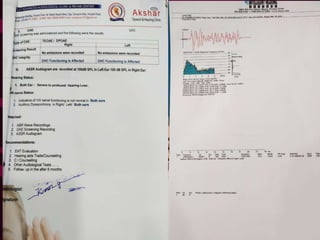


Auditory neuropathy is a hearing disorder where sound enters the inner ear normally but transmission from the inner ear to the brain is impaired. It can be caused by genetic mutations, infections, or other conditions affecting the auditory nerve. On tests, people with auditory neuropathy have normal otoacoustic emissions but abnormal or absent auditory brainstem responses and acoustic reflexes. Treatment involves hearing aids, cochlear implants, or other assistive devices to provide auditory input and support language development.



































































