Downloaded 983 times


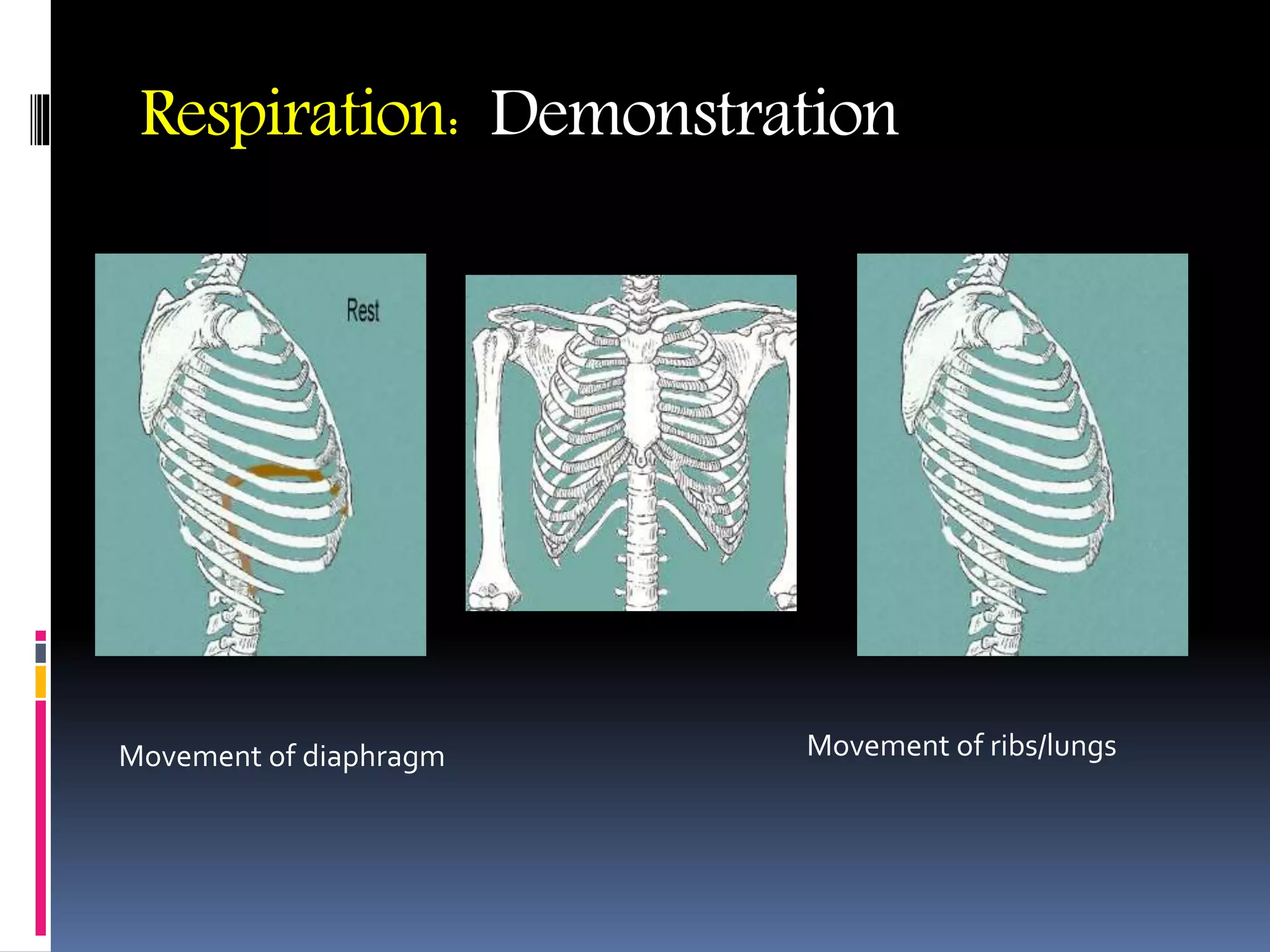









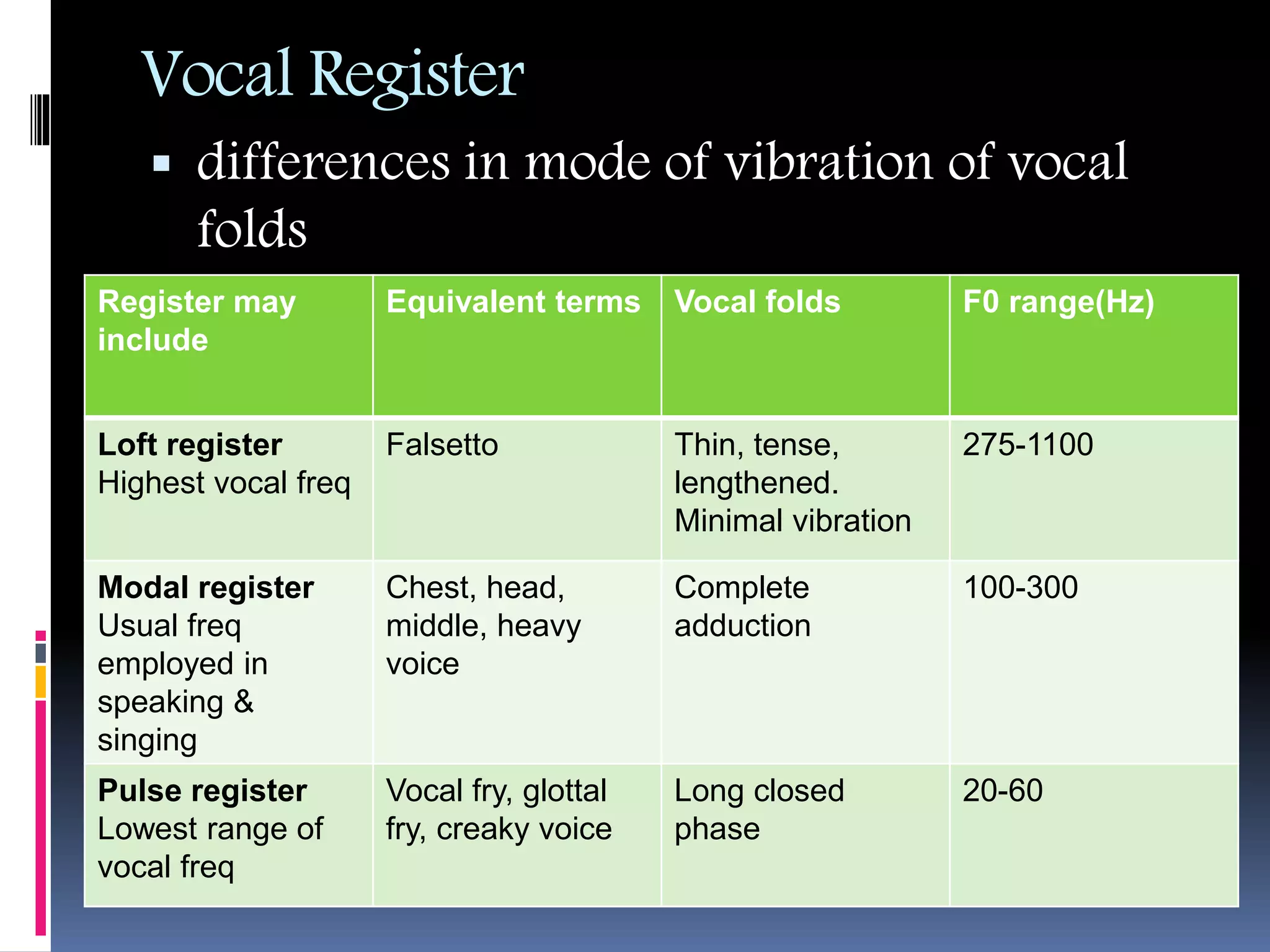







This document discusses the physiology of phonation, or voice production. It defines phonation as the rapid opening and closing of the vocal cords due to the separation and apposition of the vocal folds, accompanied by breath under lung pressure, which creates vocal sound. It describes the anatomy involved in voice production including the lungs, diaphragm, larynx, throat, mouth and nose. It discusses theories of voice production and covers topics like pitch, volume, quality, vocal registers, vocal disorders, vocal injury, and video stroboscopy.
































































































