Downloaded 830 times




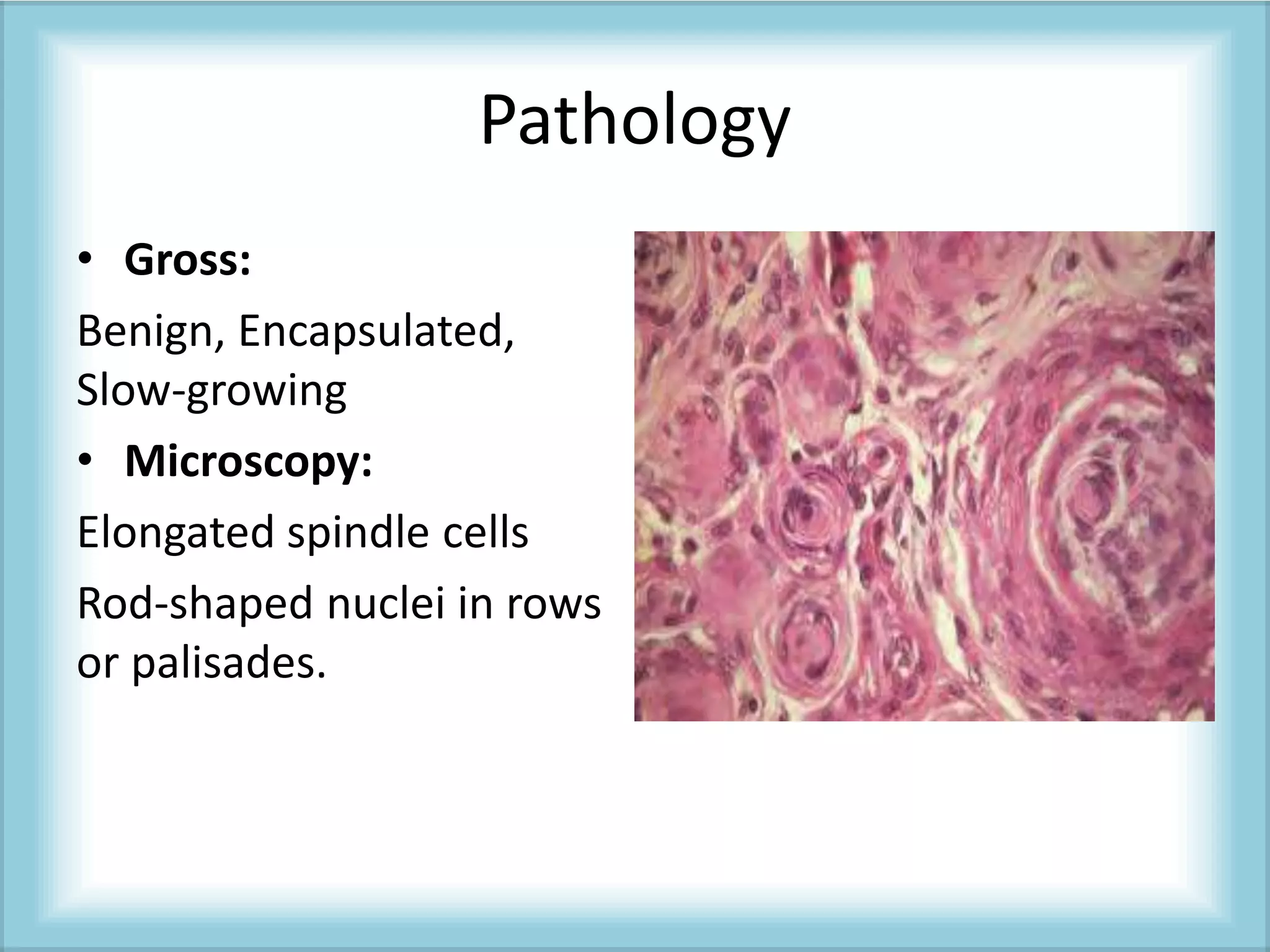








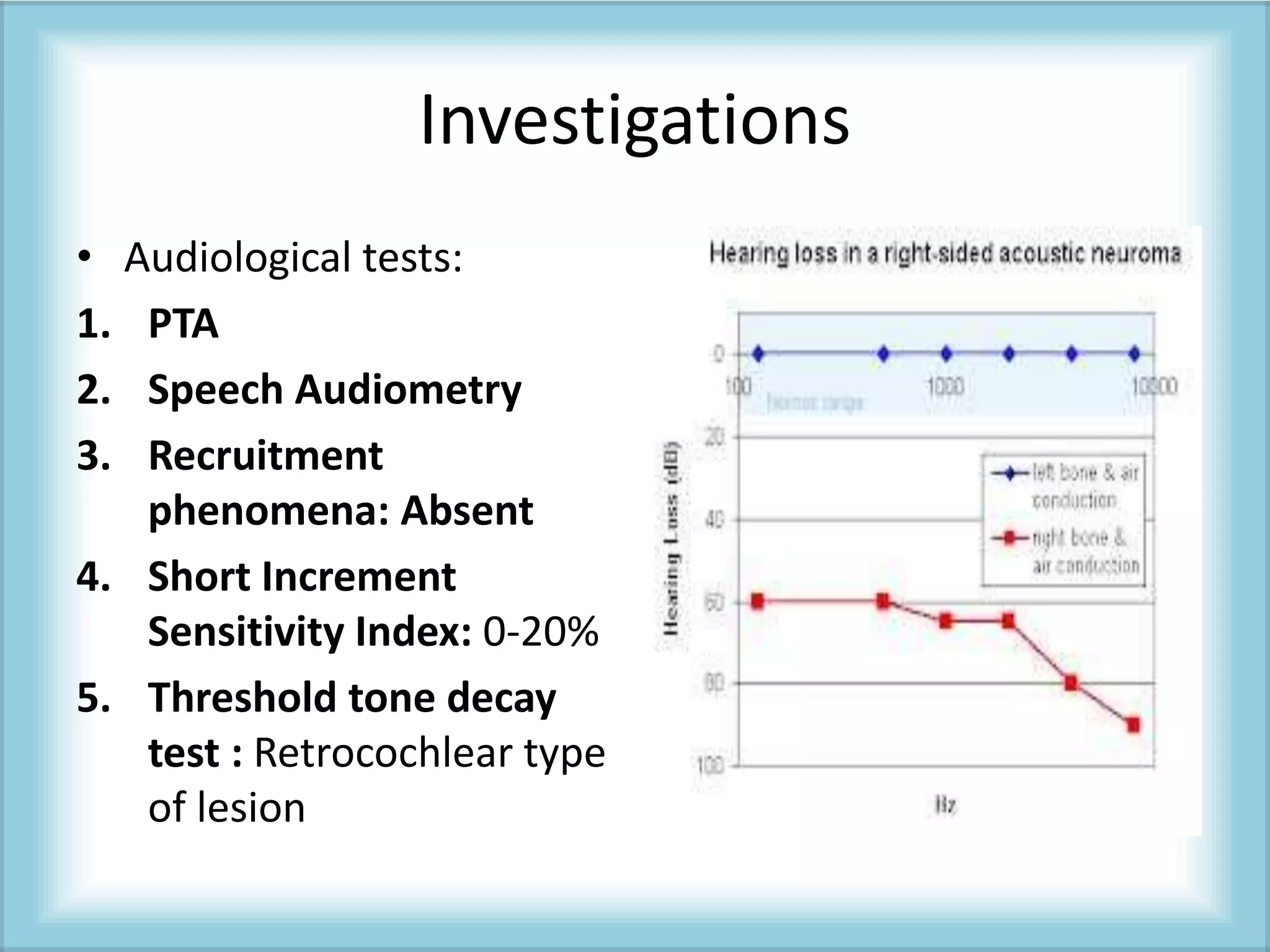















Acoustic neuroma is a benign tumor of the eighth cranial nerve. The document discusses the definition, histopathology, etiology, classification, clinical features, investigations, differential diagnosis, and management of acoustic neuroma. The key signs and symptoms include progressive hearing loss, tinnitzus, imbalance, and cranial nerve involvement including facial numbness. MRI with gadolinium is the gold standard for diagnosis. Treatment options include surgical removal via middle cranial fossa, translabyrinthine, or suboccipital approaches or stereotactic radiotherapy using gamma knife or cyber knife.

























































![ACOUSTIC NEUROMA [Autosaved].gWEGRHbRWHhpptx](https://cdn.slidesharecdn.com/ss_thumbnails/acousticneuromaautosaved-250916171936-385bbb44-thumbnail.jpg?width=640&height=640&fit=bounds)



































