Downloaded 1,612 times



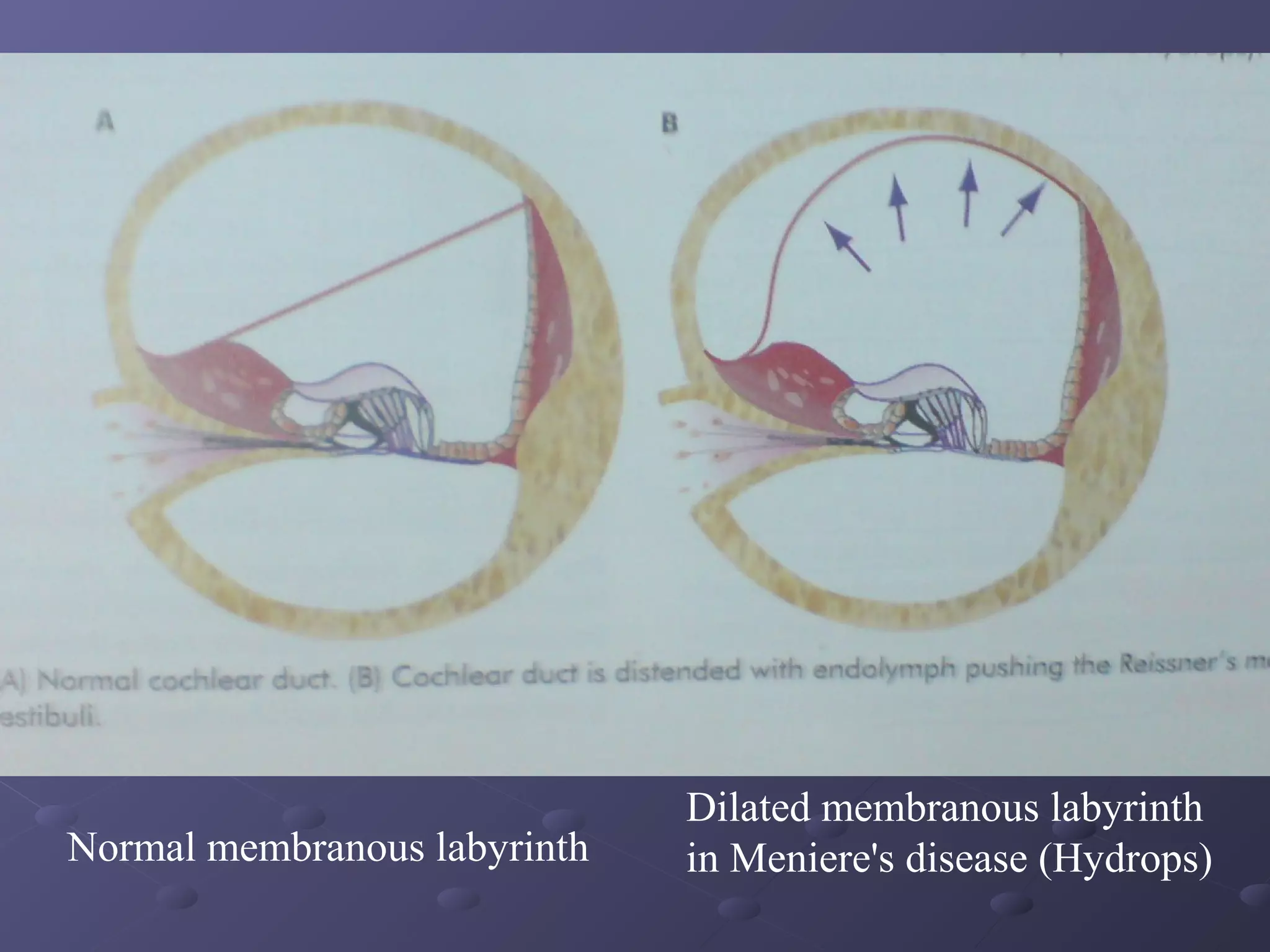


















Meniere's disease is a disorder of the inner ear that causes episodes of vertigo, hearing loss, and tinnitus. It results from endolymphatic hydrops, or a distension of the endolymphatic system in the inner ear. It typically affects people between 35-60 years old and is more common in females. Treatment involves managing symptoms during attacks and preventing future attacks. Medical treatment focuses on symptom relief through lifestyle changes, medications, and intratympanic injections. Surgical options include endolymphatic sac surgery, vestibular nerve section, ultrasonic destruction of the vestibular labyrinth, and labyrinthectomy.



































































