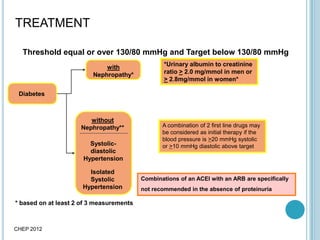
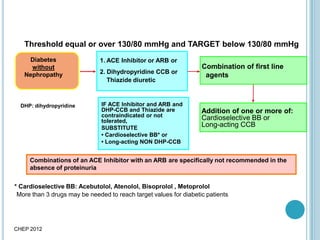
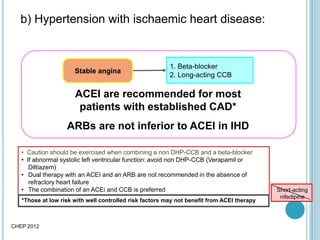
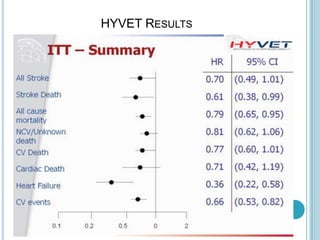
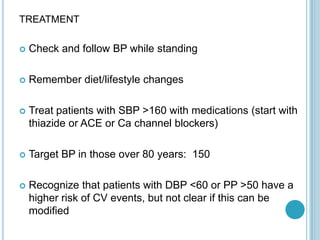
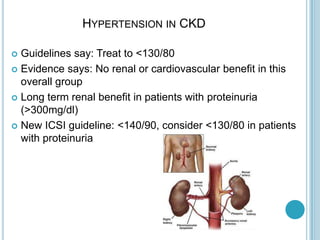
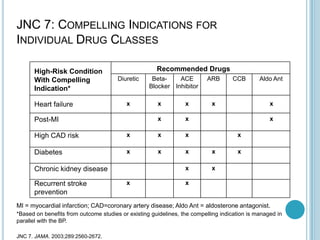
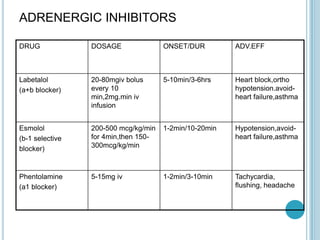
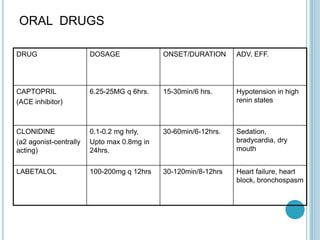
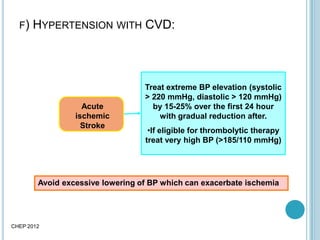
This document discusses recommendations for treating hypertension in special populations and situations. It recommends treating hypertension in patients with diabetes or chronic kidney disease to a goal of <130/80 mmHg according to JNC 7 guidelines. It provides guidance on treating hypertension in patients with diabetes, cardiovascular disease, chronic kidney disease, and the elderly. It also covers treating hypertensive emergencies and crises as well as hypertension in other situations such as pregnancy, children, and those with comorbidities like asthma. Drug classes and specific medications are suggested depending on the population and clinical situation.



![Treatment
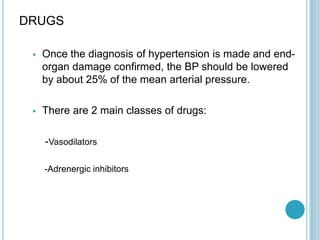
CHEP 2012
Chronic kidney
disease and
proteinuria *
ACEI/ARB:
Bilateral renal
artery stenosis
ACEI or ARB (if ACEI intolerant)
Combination with other agents
Additive therapy: Thiazide diuretic.
Alternate: If volume overload: loop diuretic
Target BP: < 140/90 mmHg
* albumin:creatinine ratio [ACR] > 30 mg/mmol
or urinary protein > 500 mg/24hr
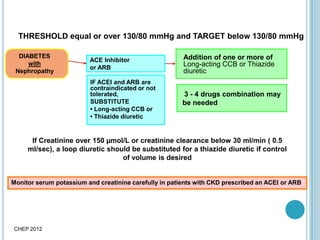
Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB
Combinations of a ACEI and a ARB are specifically not recommended in the absence of proteinuria](https://image.slidesharecdn.com/hypertension-130702024223-phpapp01/85/Hypertension-23-320.jpg)











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











