Downloaded 294 times









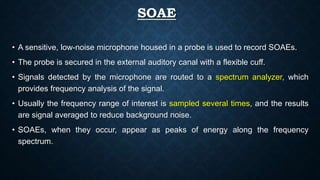











![PTA V/S OAE
• Pure-tone (PT) audiometry measures throughout the outer ear, middle ear,
cochlea, cranial nerve (CN) VIII, and central auditory system.
• OAEs measure only the peripheral auditory system, which includes the outer ear,
middle ear, and cochlea. The response only emanates from the cochlea, but the
outer and middle ear must be able to transmit the emitted sound back to the
recording microphone.
• OAEs cannot be used to fully describe an individual's auditory thresholds, but they
can help question or validate other threshold measures (eg, in suspected
functional [feigned] hearing loss), or they can provide information about the site of
the lesion.](https://image.slidesharecdn.com/otoacousticemission-190425111855/85/Otoacoustic-emission-62-320.jpg)









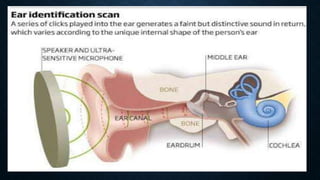



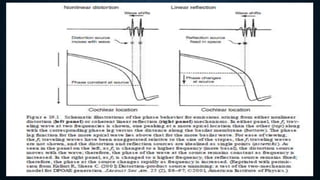
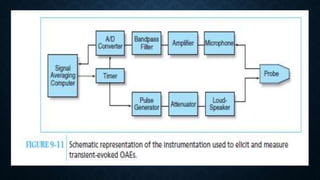
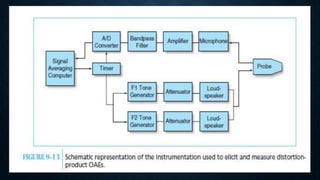
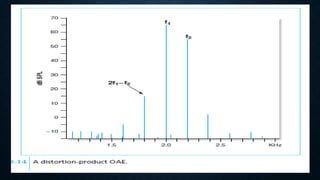
Otoacoustic emissions are low-intensity sounds generated by the inner ear that can be measured in the ear canal. They are produced by the outer hair cells' electromotility in response to sound stimulation. There are two main mechanisms that produce otoacoustic emissions - nonlinear distortion, attributed to outer hair cell action, and linear reflection from impedance mismatches in the cochlea. Measuring otoacoustic emissions can reveal the integrity of outer hair cell function. The different types of otoacoustic emissions include spontaneous, transient-evoked, distortion product, and stimulus frequency emissions.






































![Mai EchoG and OAEs ENT [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maiechogandoaesentrecovered-230503021828-debb4756-thumbnail.jpg?width=640&height=640&fit=bounds)



































