Download to read offline

![The cerebrospinal Fluid [CSF] is
a clear, colorless transparent,
tissue fluid present in the
cerebral ventricles, spinal canal,
and subarachnoid spaces.](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-2-320.jpg)










![Lateral ventricle
Foramen of Monro [Interventricular foramen]
Third ventricle:
Subarachnoid space of Brain and Spinal cord
Fourth ventricle:
Cerebral aqueduct
Foramen of megendie and formen of luschka](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-17-320.jpg)


![Increased inflammatory cells [pleocytosis] may be caused by
infectious and noninfectious processes.
Polymorphonuclear pleocytosis indicates acute suppurative
meningitis.
Mononuclear cells are seen in viral infections (meningoencephalitis,
aseptic meningitis), syphilis, neuroborreliosis, tuberculous
meningitis, multiple sclerosis, brain abscess and brain tumors.](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-20-320.jpg)

![Multiple sclerosis: CSF protein is normal or mildly increased.
Increased IgG in CSF, but not in serum [IgG/albumin index normally
10:1].
90% of MS patients have oligoclonal IgG bands in the CSF.
Oligoclonal bands occur in the CSF only not in the serum.
The CSF in MS often contains myelin fragments and myelin basic
protein (MBP).
MBP can be detected by radioimmunoassay. MBP is not specific for MS.
It can appear in any condition causing brain necrosis, including infarcts.](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-22-320.jpg)


![Xanthochromia [blonde color] of the CSF following subarachnoid
hemorrhage is due to oxyhemoglobin which appears in 4 to 6
hours and bilirubin which appears in two days.
Xanthochromia may also be seen with hemorrhagic infarcts, brain
tumors, and jaundice.](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-25-320.jpg)



![A lumbar puncture also called a spinal
tap is a procedure where a sample of
cerebrospinal fluid is taken for
examination.
CSF is mainly used to diagnose
meningitis [an infection of the
meninges].
It is also used to diagnose some other
conditions of the brain and spinal cord.](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-29-320.jpg)

![1. Material for sterile technique
[gloves and mask are necessary]
2. Spinal Needle, 20 and 22-gauge
3. Manometer
4. Three-way stopcock
5. Sterile drapes
6. 1% lidocaine without epinephrine in
a 5-cc syringe with a 22 and 25-
gauge needles
7. Material for skin sterilization
8. Adhesive dressing](https://image.slidesharecdn.com/csf-200830144749/85/Csf-cerebro-spinal-fluid-31-320.jpg)













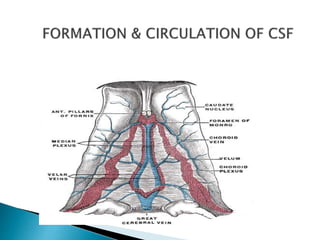
Cerebrospinal fluid (CSF) is a clear fluid produced by the choroid plexuses in the brain ventricles and circulates through the ventricular system before reabsorbing into the venous blood. CSF acts as a cushion and protects the brain, and its analysis through lumbar puncture can help diagnose conditions like meningitis, tumors, and other brain and spinal disorders. The procedure involves inserting a needle between vertebrae to collect CSF for examination of properties like pressure, cells, proteins, and chemicals.









































































