Downloaded 162 times
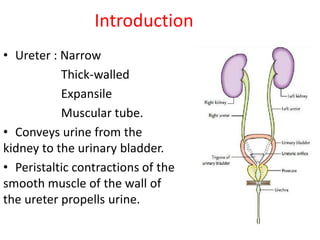
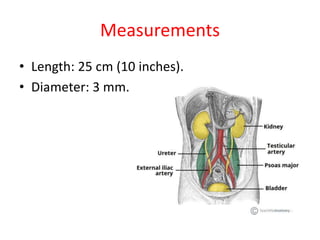
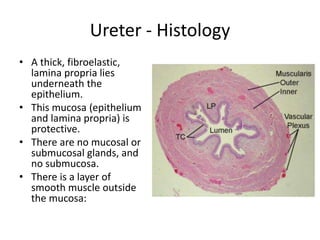
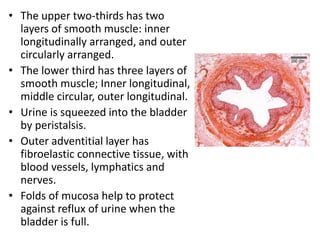
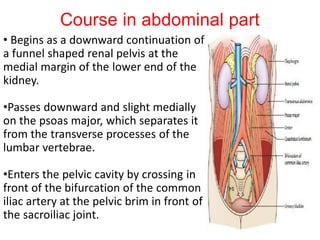
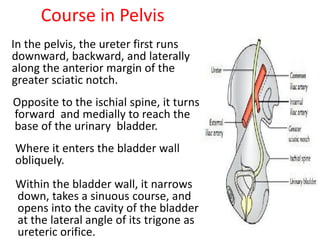
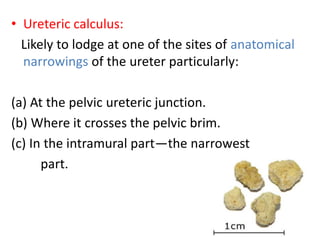


The ureter is a narrow, thick-walled, muscular tube that conveys urine from the kidney to the urinary bladder. Peristaltic contractions of the smooth muscle in the ureter wall propel urine downward. The ureter has three layers of smooth muscle in the lower third and two layers in the upper two-thirds. It courses down the posterior abdominal wall and enters the pelvis, where it crosses the common iliac artery. In the pelvis, it travels laterally along the sciatic notch before entering the bladder obliquely. The ureter has several sites of anatomical narrowing where stones are prone to lodge, including at the pelvic brim and ure





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















