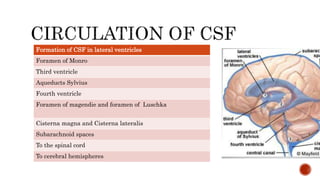
Cerebrospinal fluid (CSF) is a clear, colorless fluid that surrounds the brain and spinal cord, produced by the choroid plexus at a rate of approximately 0.3 ml/min, with an average volume of 150 ml. CSF acts as a buffer, protects the brain from trauma, and facilitates the exchange of nutrients and waste products between blood and brain tissue, with a complex absorption process primarily occurring through arachnoid villi. Abnormalities in CSF accumulation can lead to conditions such as hydrocephalus, which presents with symptoms such as headache, vomiting, mental weakness, and gait instability.