Downloaded 47 times

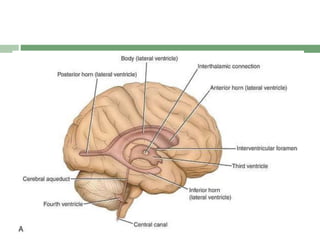
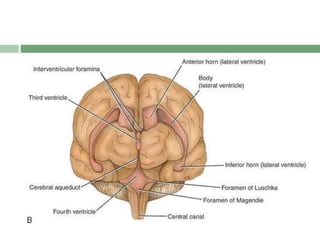
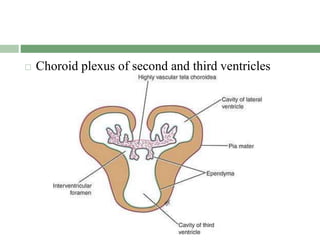
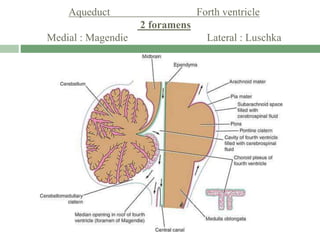
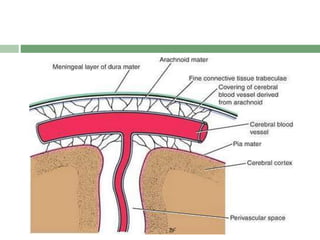
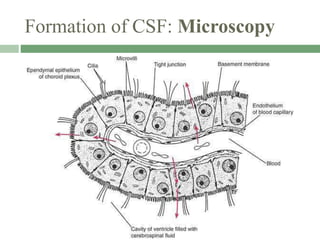
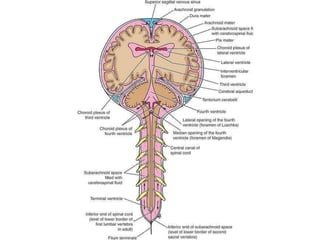
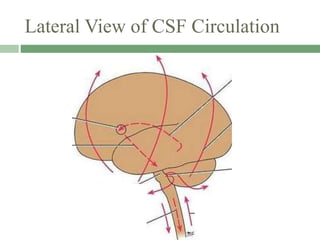
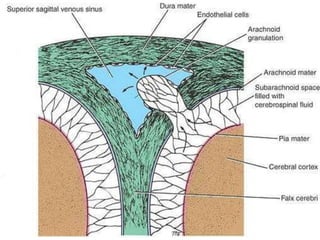
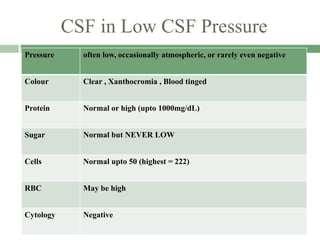
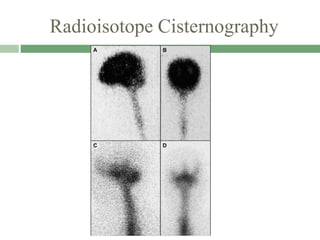
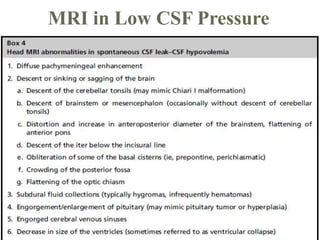
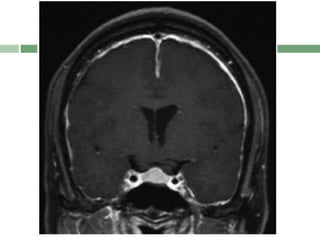
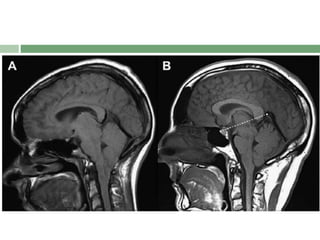
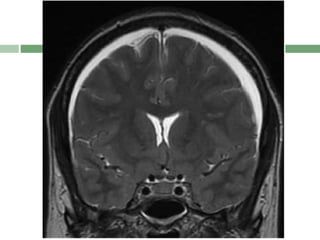
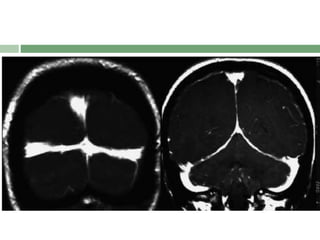
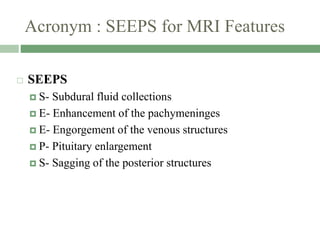
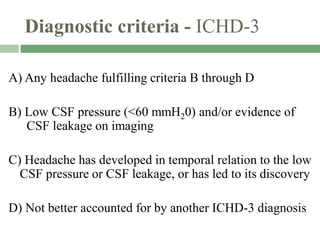
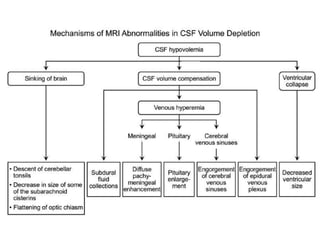
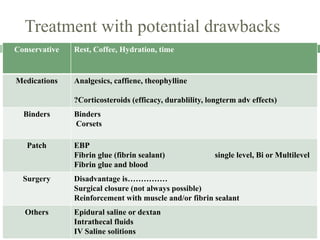
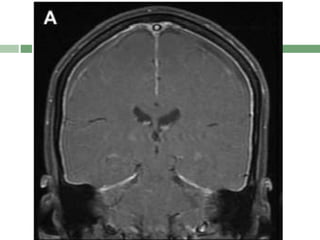



This document discusses CSF circulation and low pressure headaches. It begins by describing the anatomy of the ventricular system and subarachnoid space. CSF is produced in the choroid plexus and circulates through the ventricles and subarachnoid space before being reabsorbed. Low CSF pressure headaches can be caused by CSF leaks or hypovolemia. Symptoms include orthostatic or exertional headaches. MRI may show subdural fluid collections, pachymeningeal enhancement, venous engorgement, and sagging of posterior structures. Diagnosis is based on low CSF pressure on lumbar puncture with headaches related to the low pressure. Treatment options include conservative measures, medications, patches, fibrin




























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










