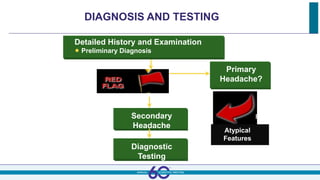
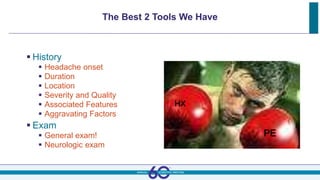
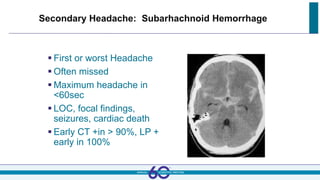
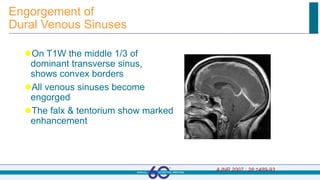
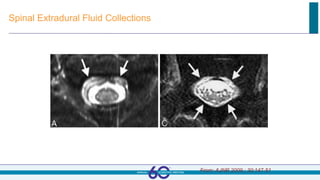
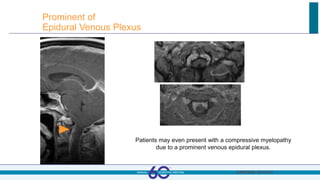
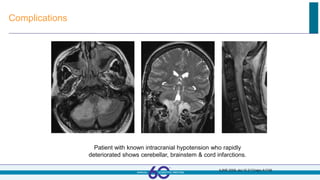
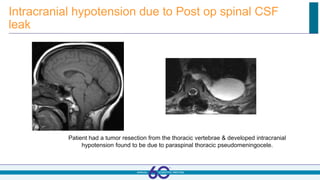
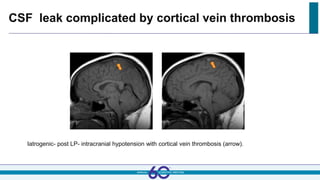
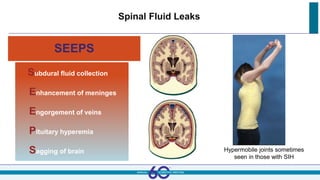
This document discusses secondary headaches from various causes. It begins with learning objectives around recognizing red flags for secondary headaches, diagnosing and managing dangerous headaches, and reviewing less common headache disorders. It then covers approaches to diagnosis like history and exam, provides examples of things to look for in the history with an acronym, and discusses limitations of CT. Several specific secondary headache disorders are discussed in depth, including vascular causes like subarachnoid hemorrhage, pseudotumor cerebri, and giant cell arteritis. Spinal fluid disorders causing headaches like post-dural puncture headache and spontaneous CSF leaks are also reviewed. Finally, headaches from CNS infections such as meningitis, brain abscess, and le