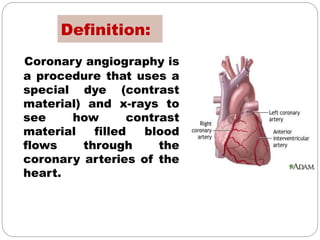
Coronary angiography is a procedure that uses dye and x-rays to see how blood flows through the coronary arteries of the heart. It is the gold standard for evaluating coronary artery disease and can identify the location and severity of any blockages. A coronary angiogram involves inserting a catheter into the heart and injecting dye so that blockages are highlighted on x-ray images. Potential complications are usually minor but can include heart attack, stroke, or kidney injury from the dye. The results of the angiogram are used to determine if further procedures like angioplasty or bypass surgery are needed.