Downloaded 30 times

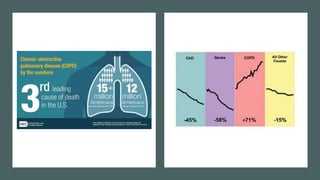
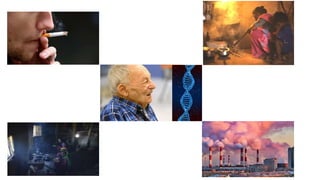


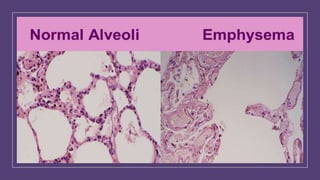
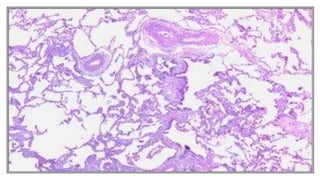

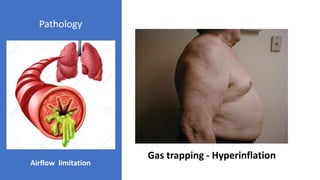
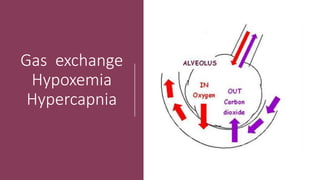


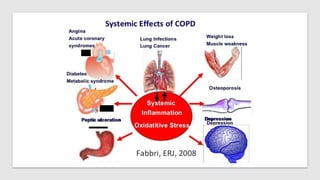
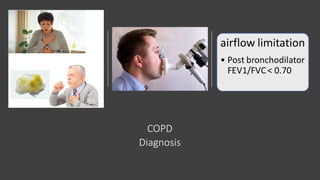
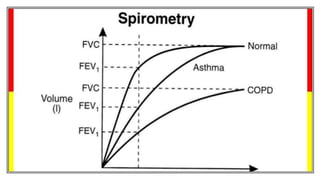
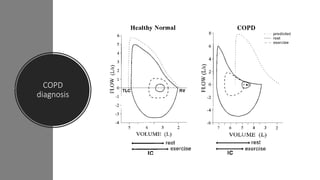

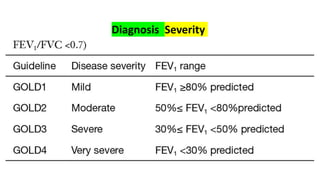
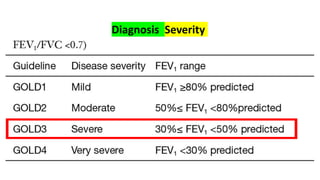



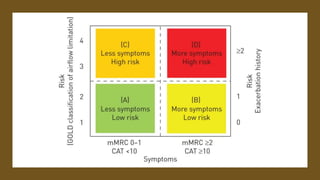
















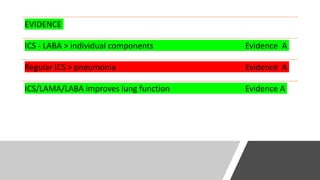
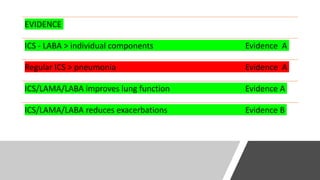








This document discusses COPD (chronic obstructive pulmonary disease), including its definition, symptoms, pathology, diagnosis, management, and treatment. Some key points include: - COPD is characterized by persistent respiratory symptoms and airflow limitation usually caused by significant exposure to noxious particles or gases. It involves chronic inflammation in the airways, lung parenchyma, and pulmonary vasculature. - Diagnosis is based on spirometry showing airflow limitation that is not fully reversible. Severity is classified based on lung function tests and exacerbation history. - Management focuses on smoking cessation, vaccinations, pulmonary rehabilitation, pharmacologic therapy including bronchodilators and inhaled corticosteroids,












































































