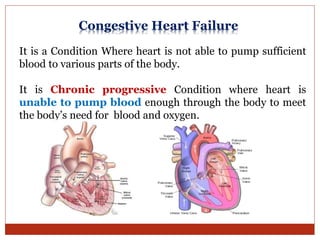
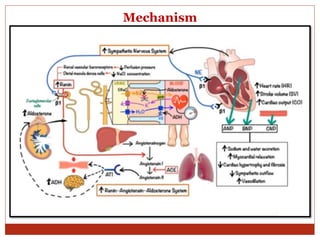
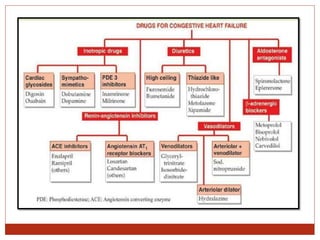
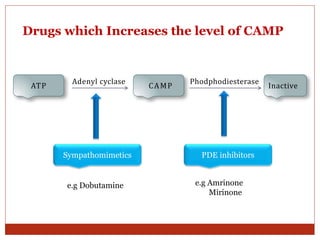
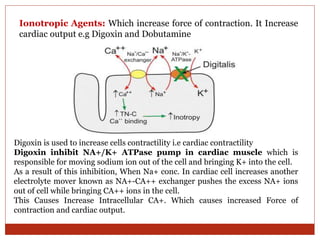
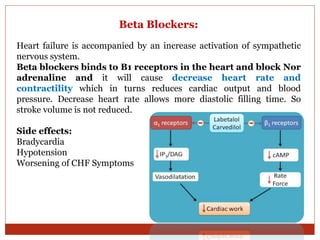
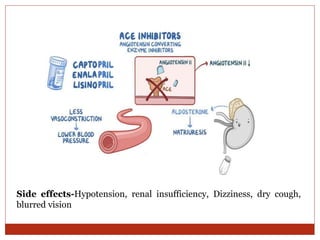
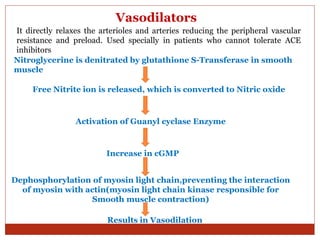
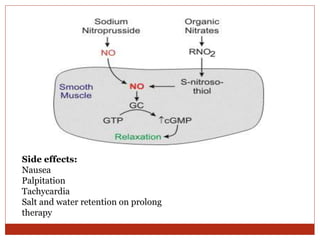
This document discusses congestive heart failure (CHF), which occurs when the heart cannot pump enough blood to meet the body's needs. It defines two types of CHF based on ejection fraction - systolic and diastolic dysfunction. Several causes of CHF are listed, including arrhythmias, myocardial infarction, hypertension, and obesity. The body compensates via the sympathetic nervous system and renin-angiotensin-aldosterone system. Drug classes used to treat CHF are discussed in detail, including cardiac glycosides like digoxin, beta blockers, ACE inhibitors, angiotensin receptor blockers, aldosterone antagonists, and vasodilators. Side effects of each class are