Downloaded 19 times


![References• Bauer V, Aleric Z, Jancic E, Knezevicc B, Prpicc D, Kacavendac A Subjective and perceptual analysis of voice quality
and relationship with neurological disfunction in multiple sclerosis patients Clinical Neurology and Neurosurgery
115S (2013) S17–S20
• Baylor C, Yorkston K, Bamer A, Britton D, Amtmann D Variables associated with communicative participation in
peoplewith multiple sclerosis: A regression analysis Am J Speech Lang Pathol. 2010 May ; 19(2): 143–153
• Baylor C, Yorkston K , Eadie T, Kim J, Chung H, Amtmann D The Communicative Participation Item Bank (CPIB): Item
bank calibration and development of a disorder-generic short formJ Speech Lang Hear Res. 2013 Aug; 56(4):
1190–1208
• Beukelman, D. R., Kraft, G. H., & Freal, J. Expressive communication disorders in persons with multiple sclerosis.
Archives of Physical Medicine and Rehabilitation (1985) 66 675–677
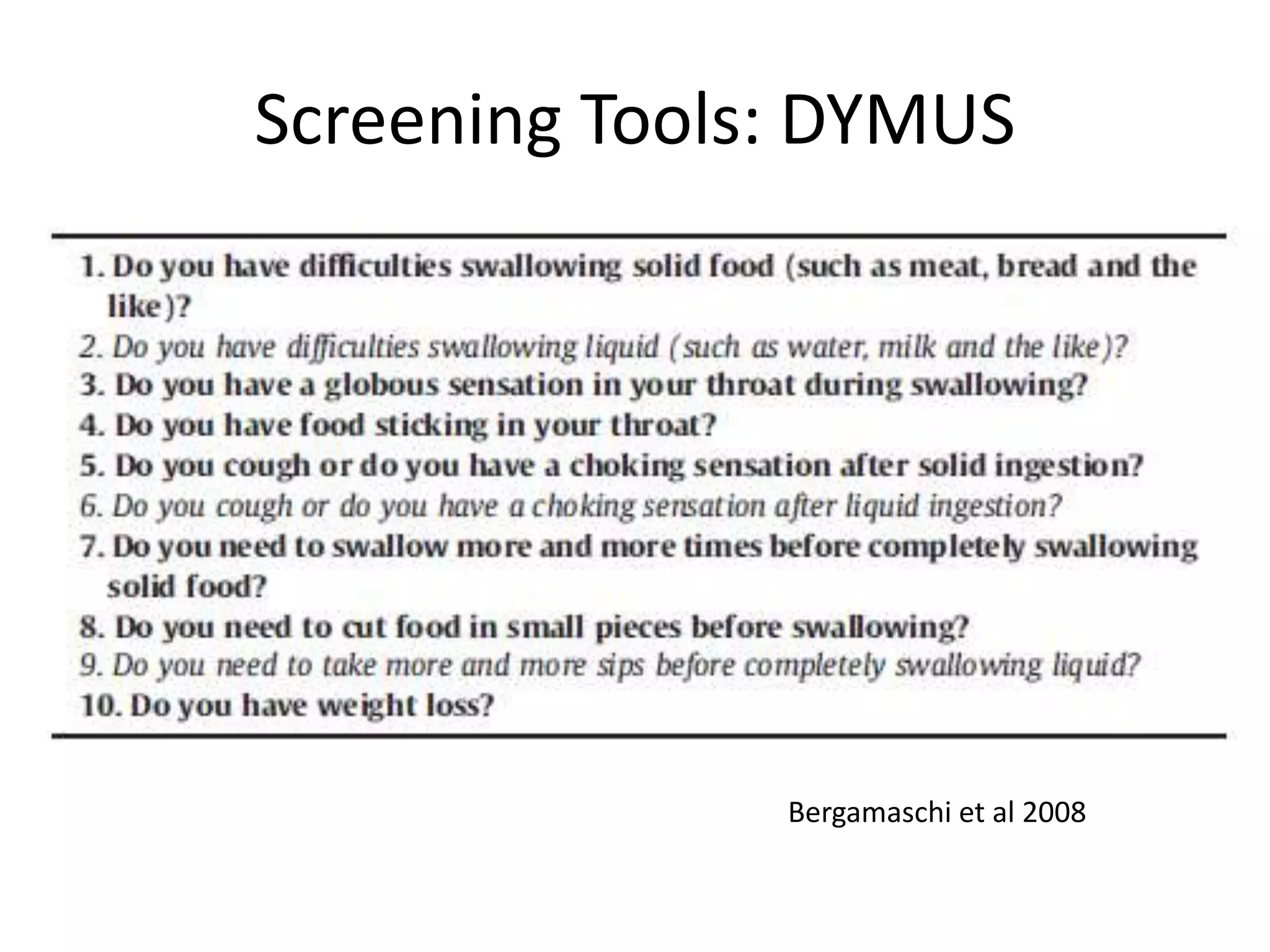
• Bergamaschi R The DYMUS questionnaire for the assessment of dysphagia in multiple sclerosis Journal of the
Neurological Sciences 269 (2008) 49-53
• Bringfelt PA, Hartelius L, Runmarker B Communication Problems in Multiple Sclerosis: 9-Year Follow-Up Int J MS
Care 2006;8:130–140.
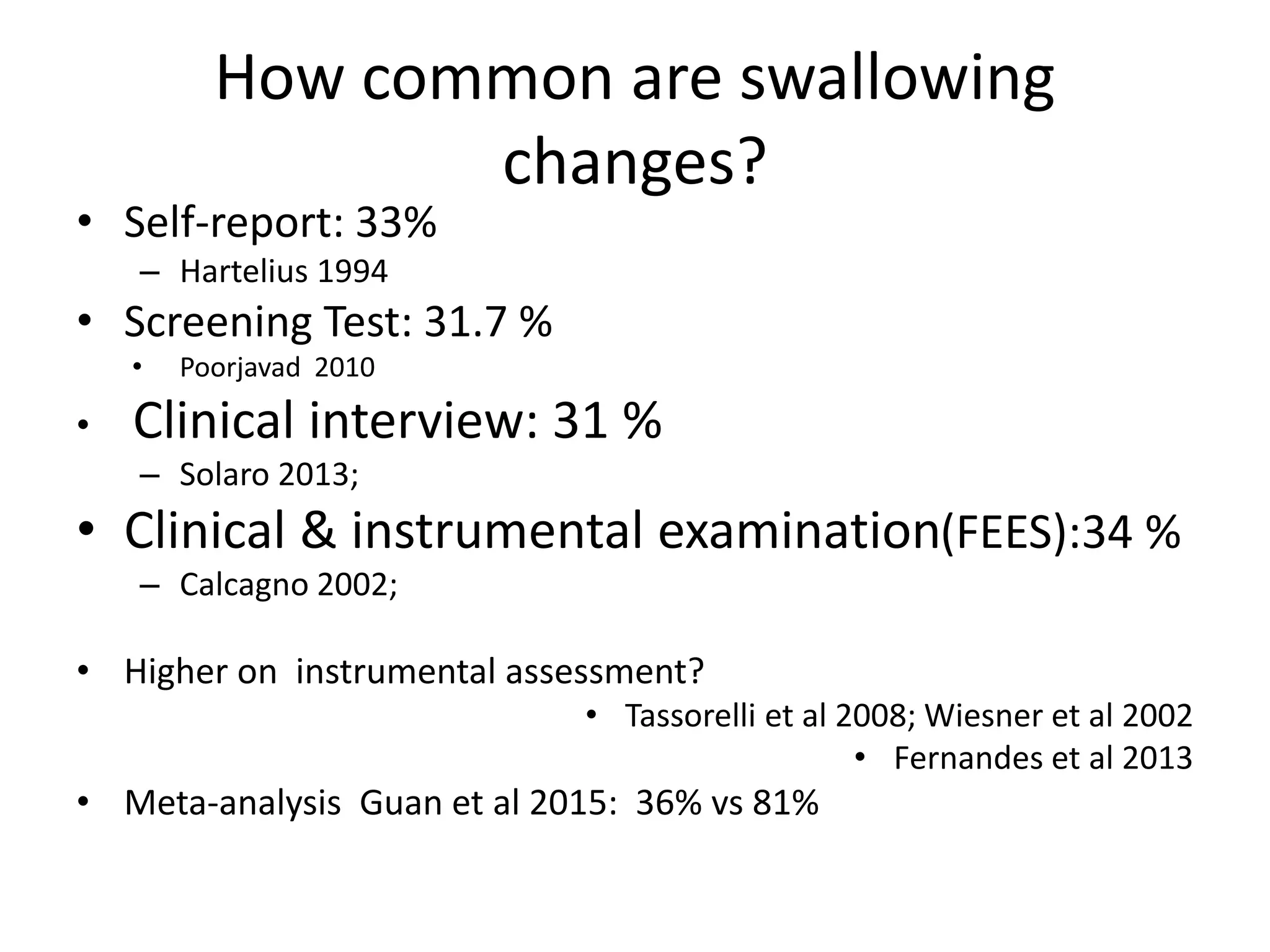
• Calcagno P, Ruoppolo G, Grasso MG, De Vincentiis M, Paolucci S. Dysphagia in multiple sclerosis - prevalence and
prognostic factors. Acta Neurol. Scand. [2002]
• Bülow M, Olsson R, Ekberg O. Videoradio-graphic analysis of how carbonated thin liquids and thickened liquids
affect the physiology of swallowing in subjects with aspiration on thin liquids. Acta Radiologica. 2003;44:366–372
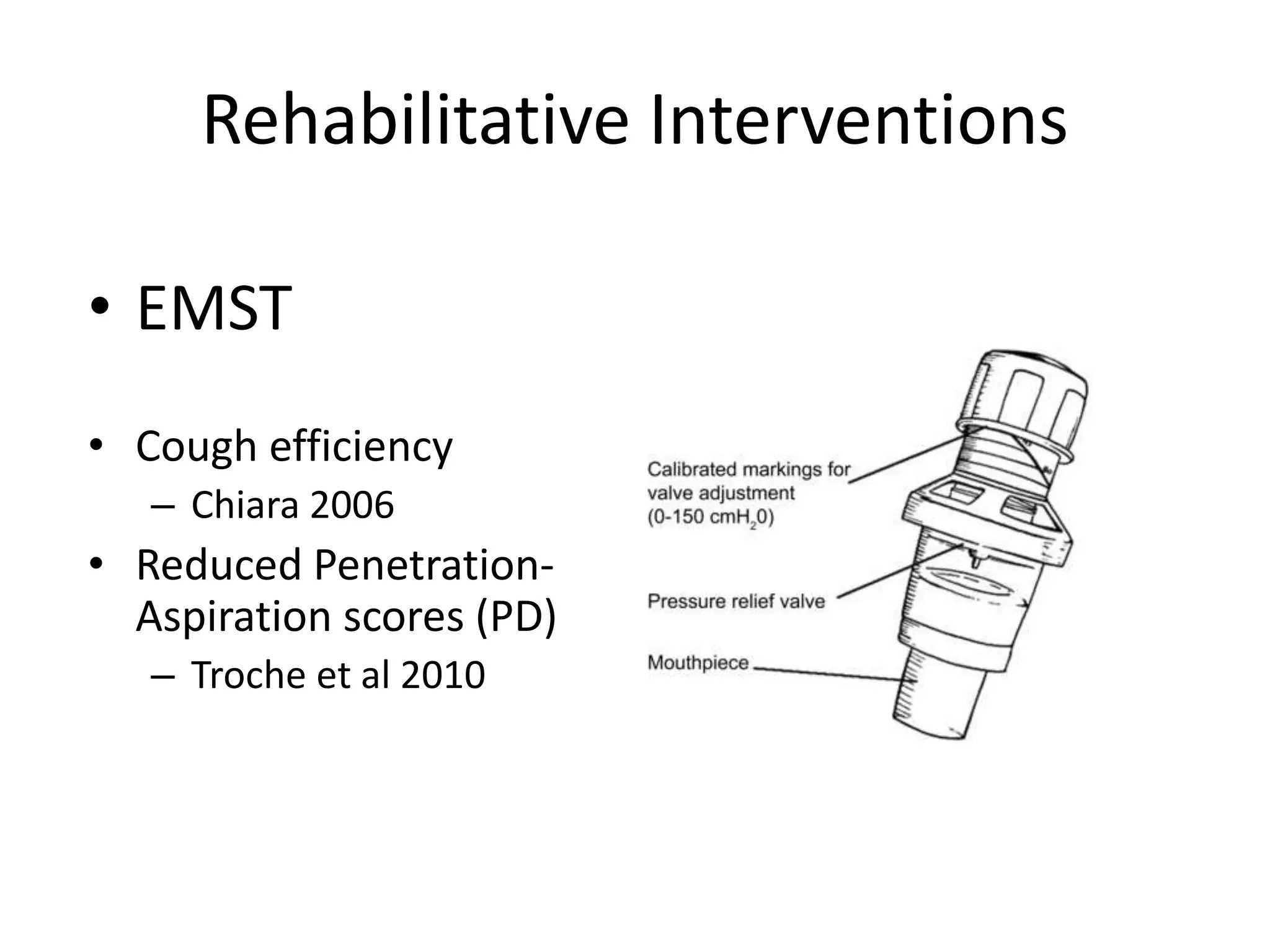
• Chiara T, Martin D, Davenport P, Bolser D. Expiratory muscle strength training in persons with multiple sclerosis
having mild to moderate disability: effect on maximal expiratory pressure, pulmonary function, and maximal
voluntary cough. Arch Phys Med Rehabil 2006;87:468–473
• Chiara, T., Martin, D., Sapienza, C. Expiratory muscle strength training: speech production outcomes in patients
with multiple sclerosis. Neurorehabil Neural Repair. 2007;21:239–249
• Clave P, Arreola V, Romea M, Medina L, Palomera E, Serra-Prat M. Accuracy of the volume-viscosity
swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin Nut 2008; 27: 806–15
• Darley FL, Brown JR, Goldstein NP Dysarthria in multiple sclerosis. J Speech Hear Res. 1972 Jun;15(2):229-45.
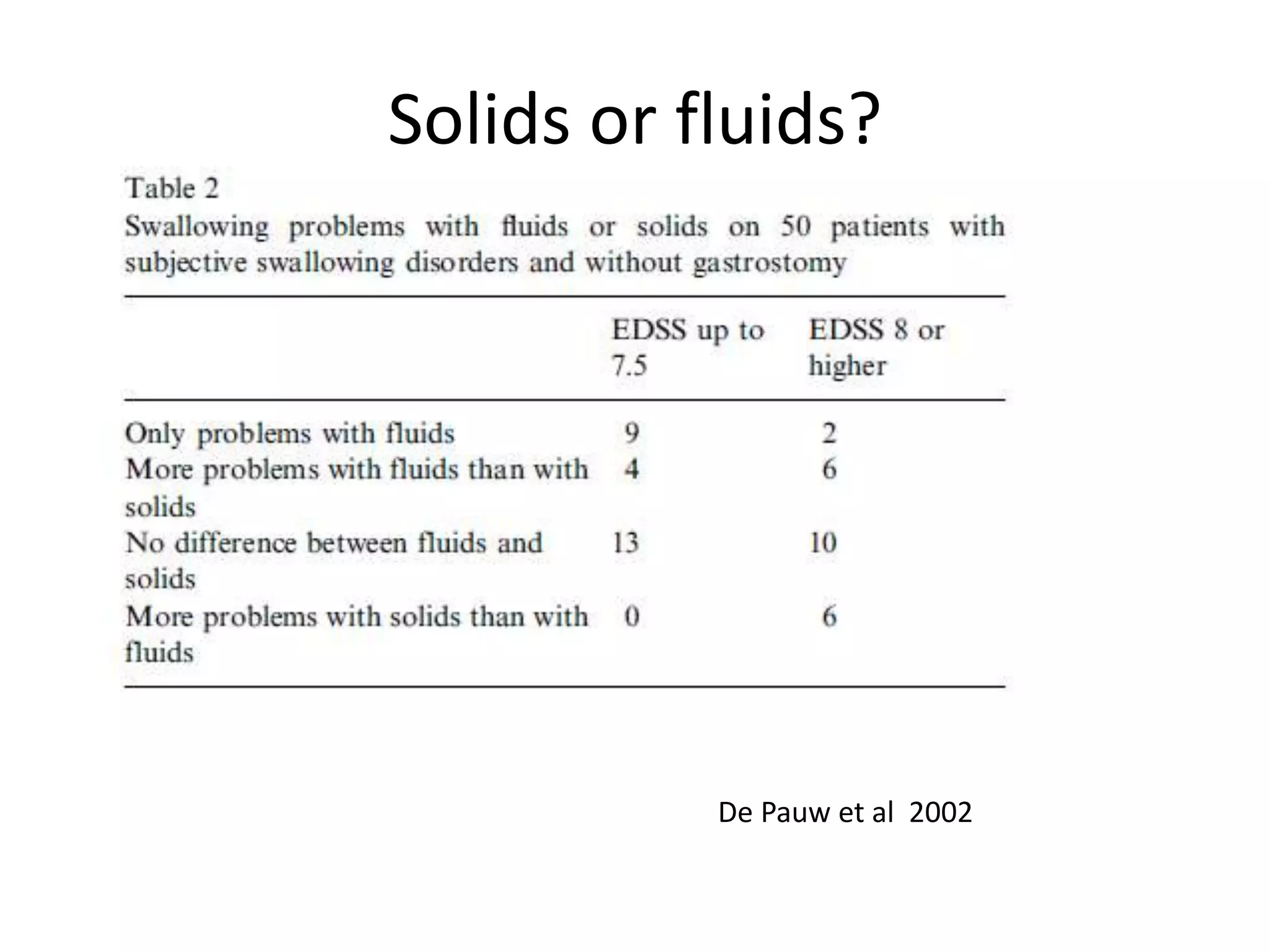
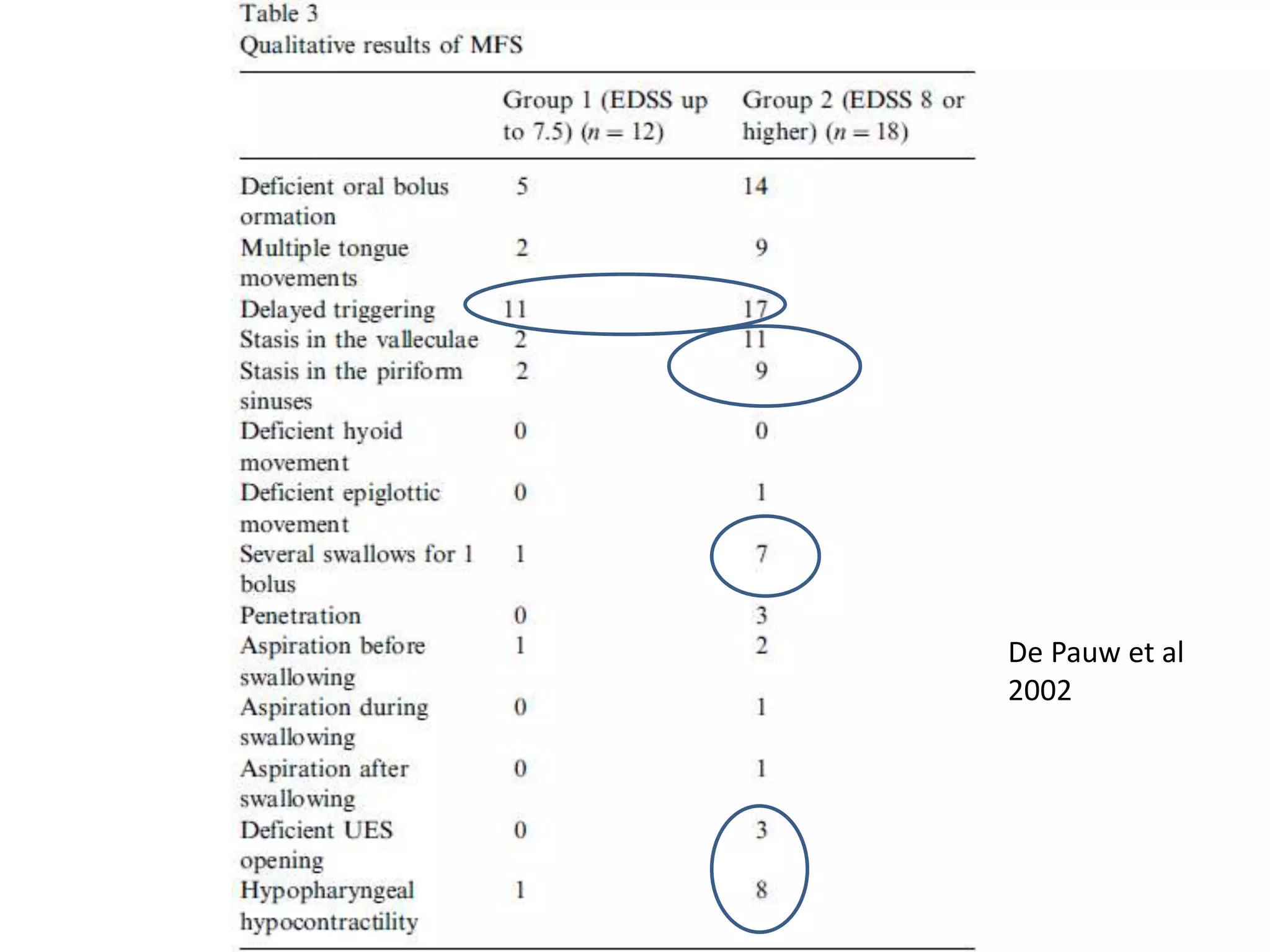
• De Pauw A, Dejaeger E, D'hooghe B, Carton H Dysphagia in multiple sclerosis Clinical neurology and neurosurgery
2002 Sep;104(4):345-51
• Dogan M, Midi I, Yazici MA, et al. Objective and subjective evaluation of voice quality in multiple sclerosis. J Voice
2007;21(6):735–40.](https://image.slidesharecdn.com/melissaloucascommunicationswallowinginms-151117110411-lva1-app6891/75/Communication-and-swallowing-in-MS-What-works-54-2048.jpg)

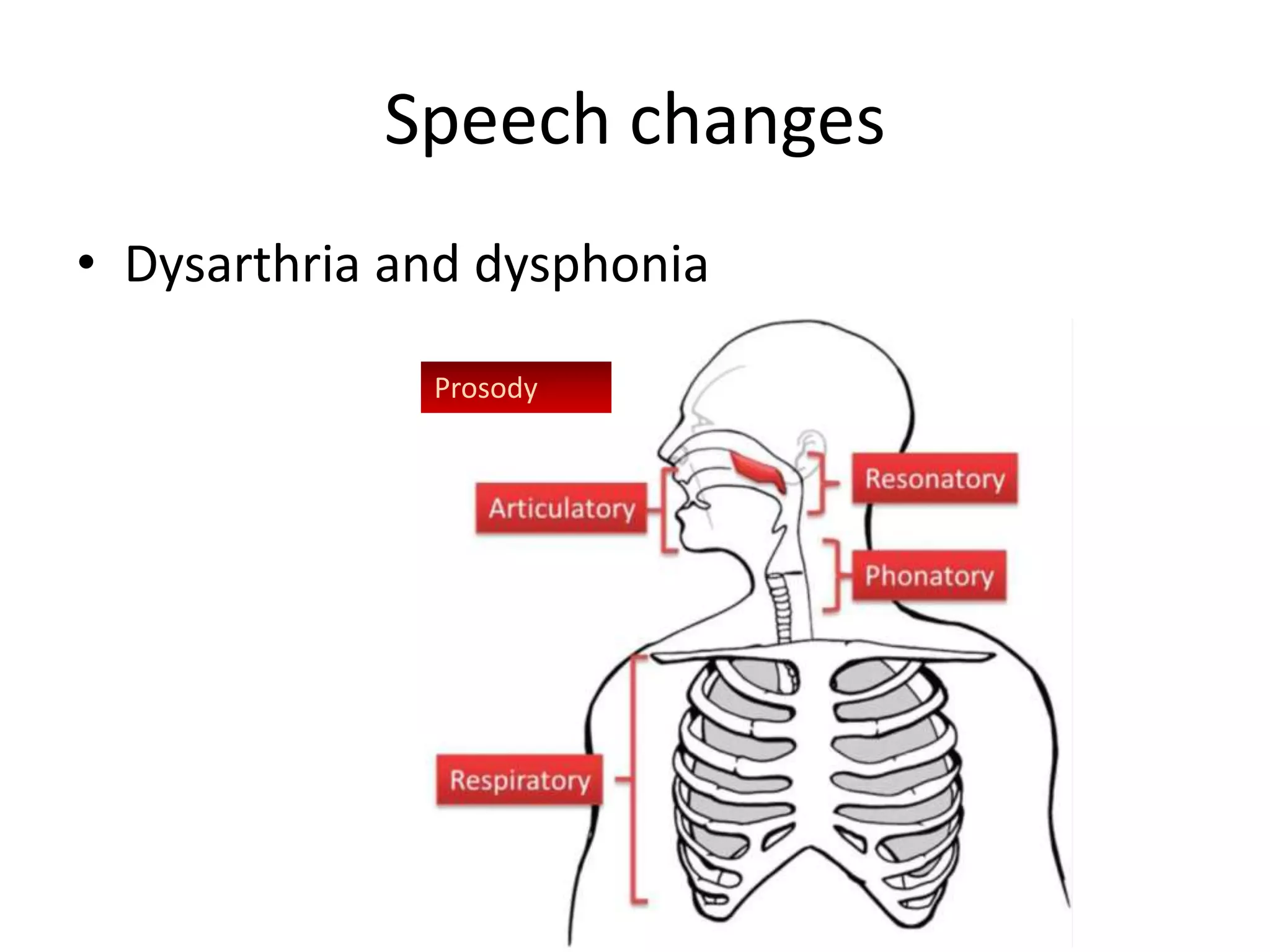
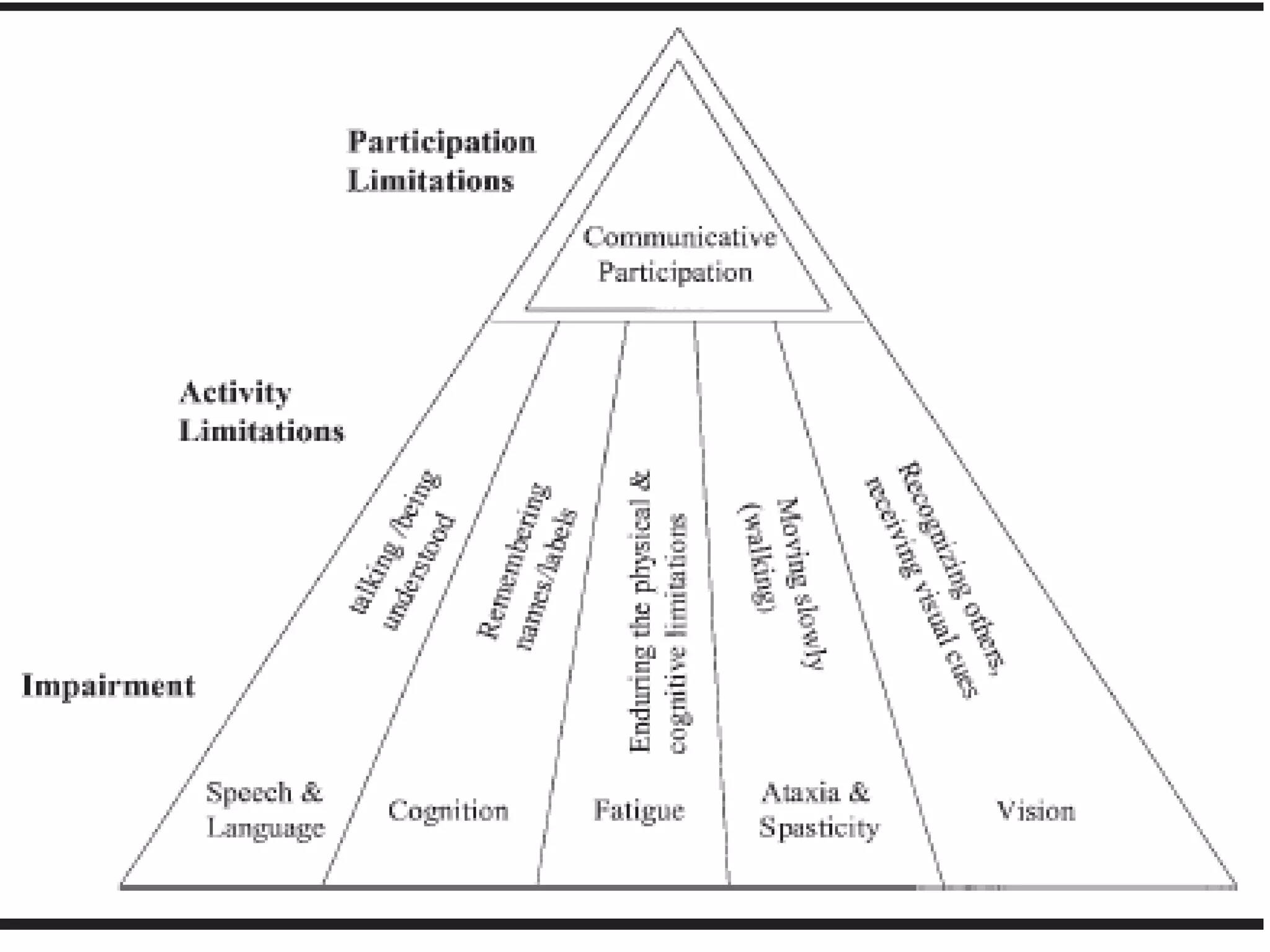
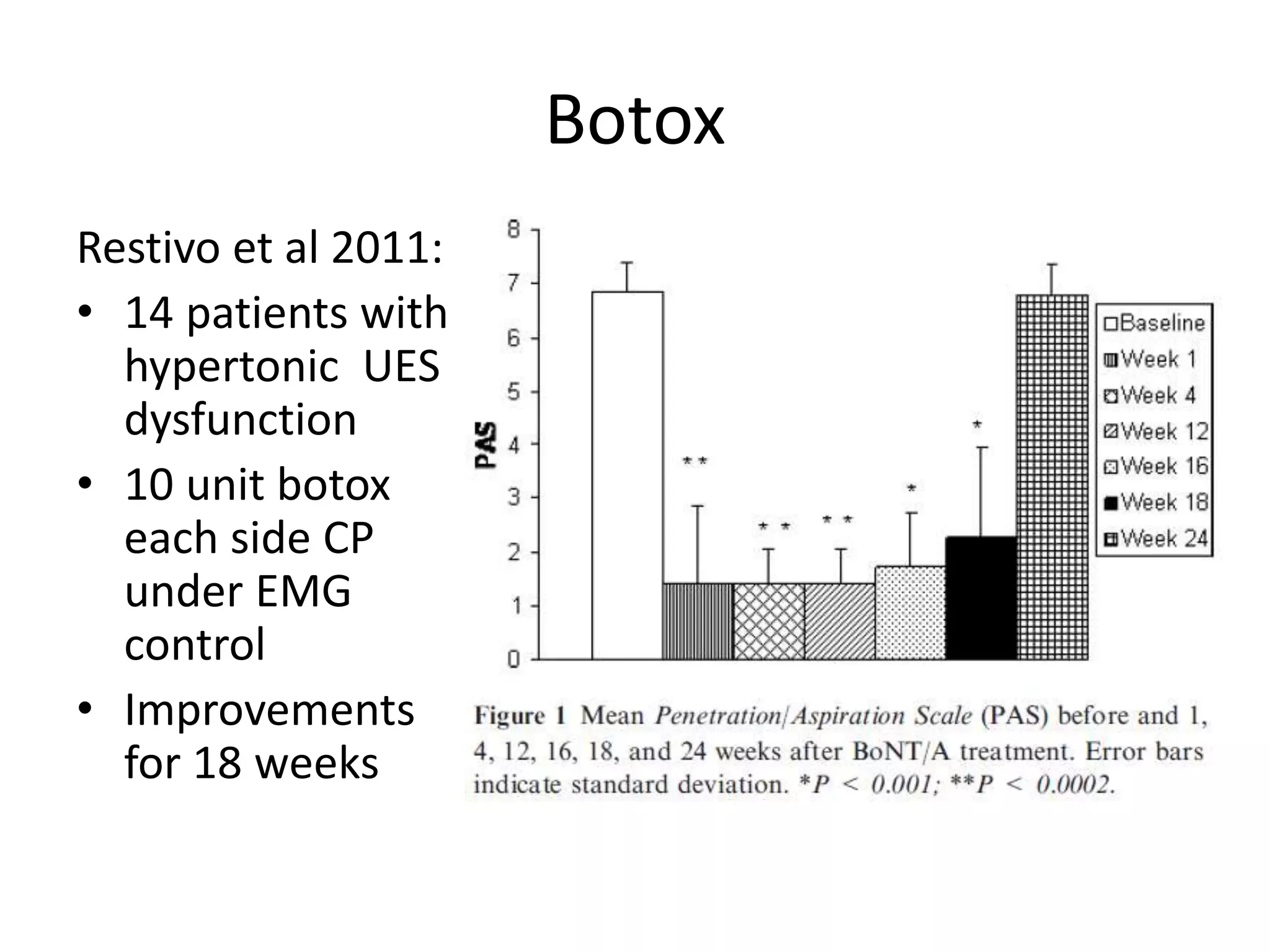
This document provides an overview of communication and swallowing issues in multiple sclerosis (MS), including characteristics, identification, and interventions. It summarizes that speech and swallowing changes are common in MS, affecting over 30% of patients, and are more likely with increased disease severity and progression. A variety of screening tools and assessments are available to identify speech and swallowing issues. Interventions can target impairment, compensation, and participation, and involve speech language therapy as well as a multidisciplinary approach. Early intervention may provide benefits, though evidence for treatments is still limited.










































































































