Download to read offline


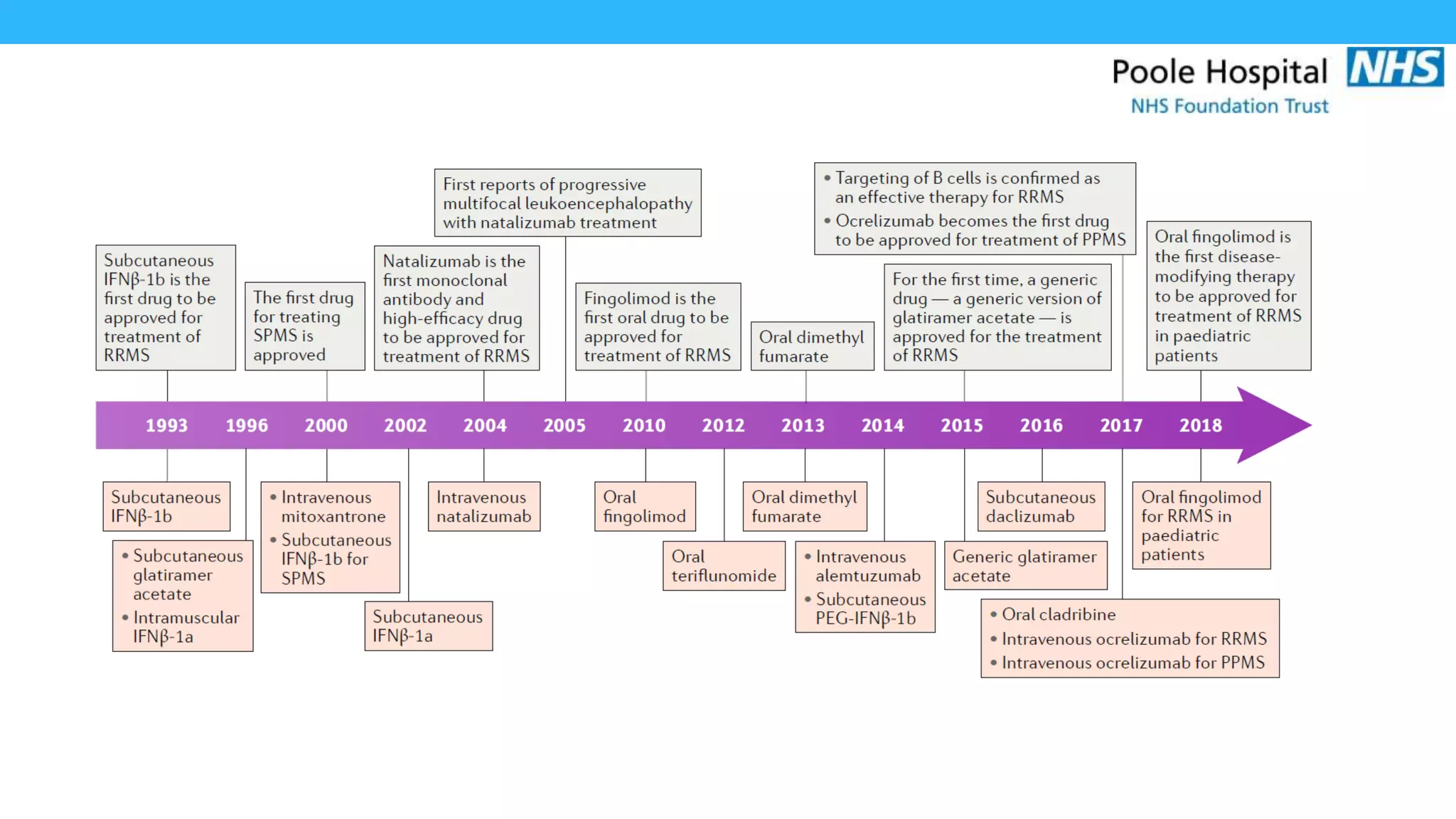




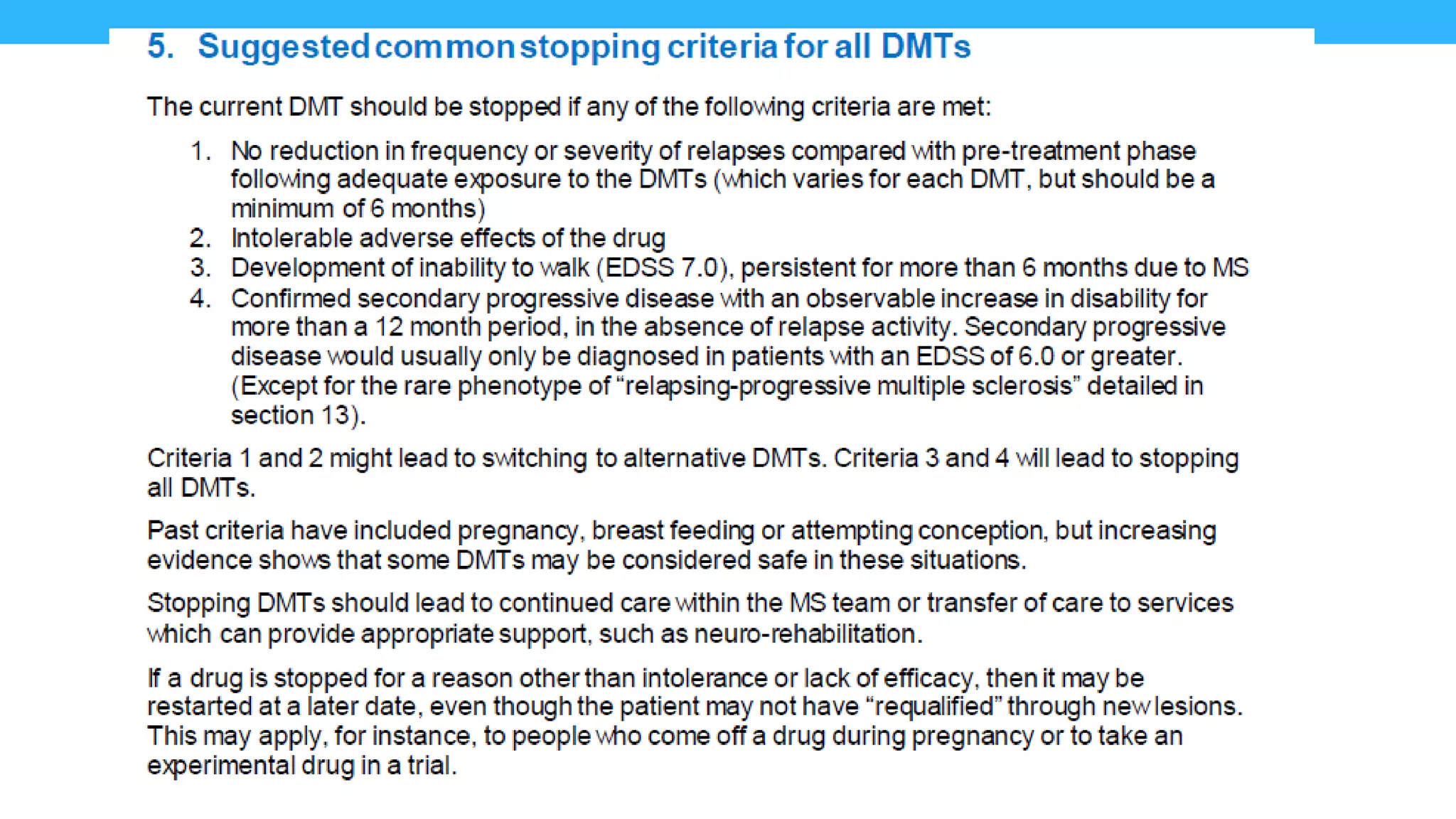



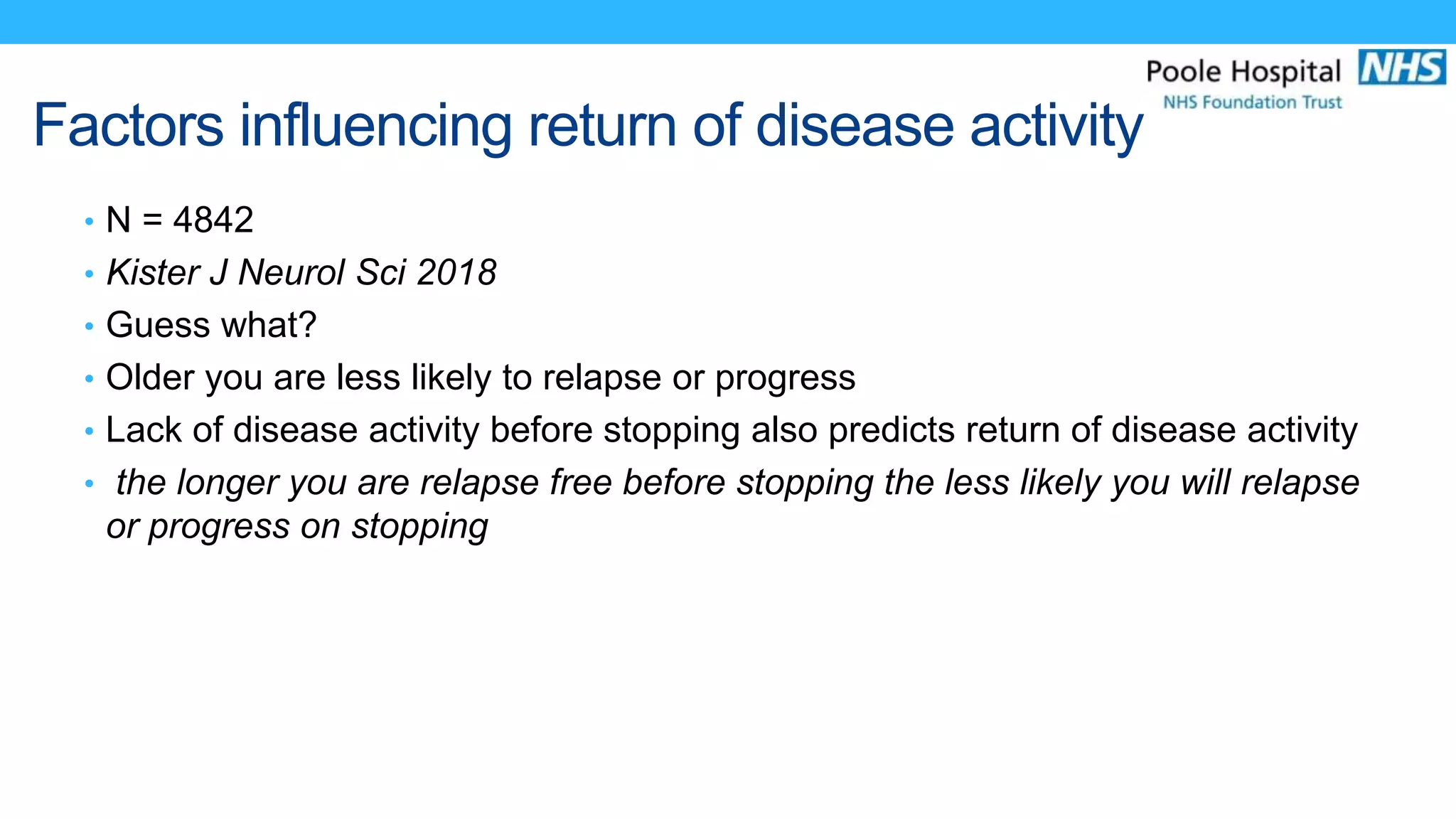


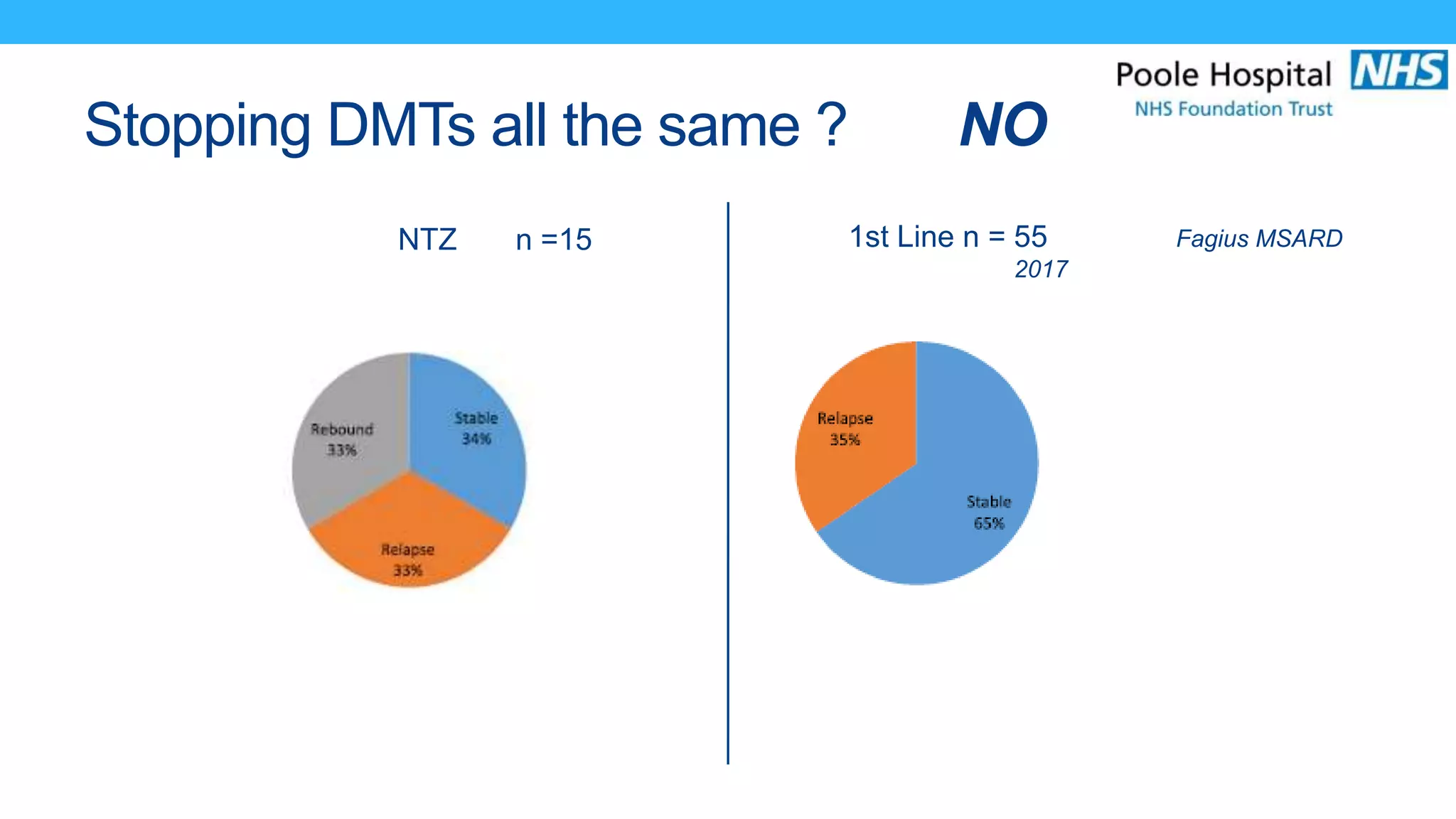



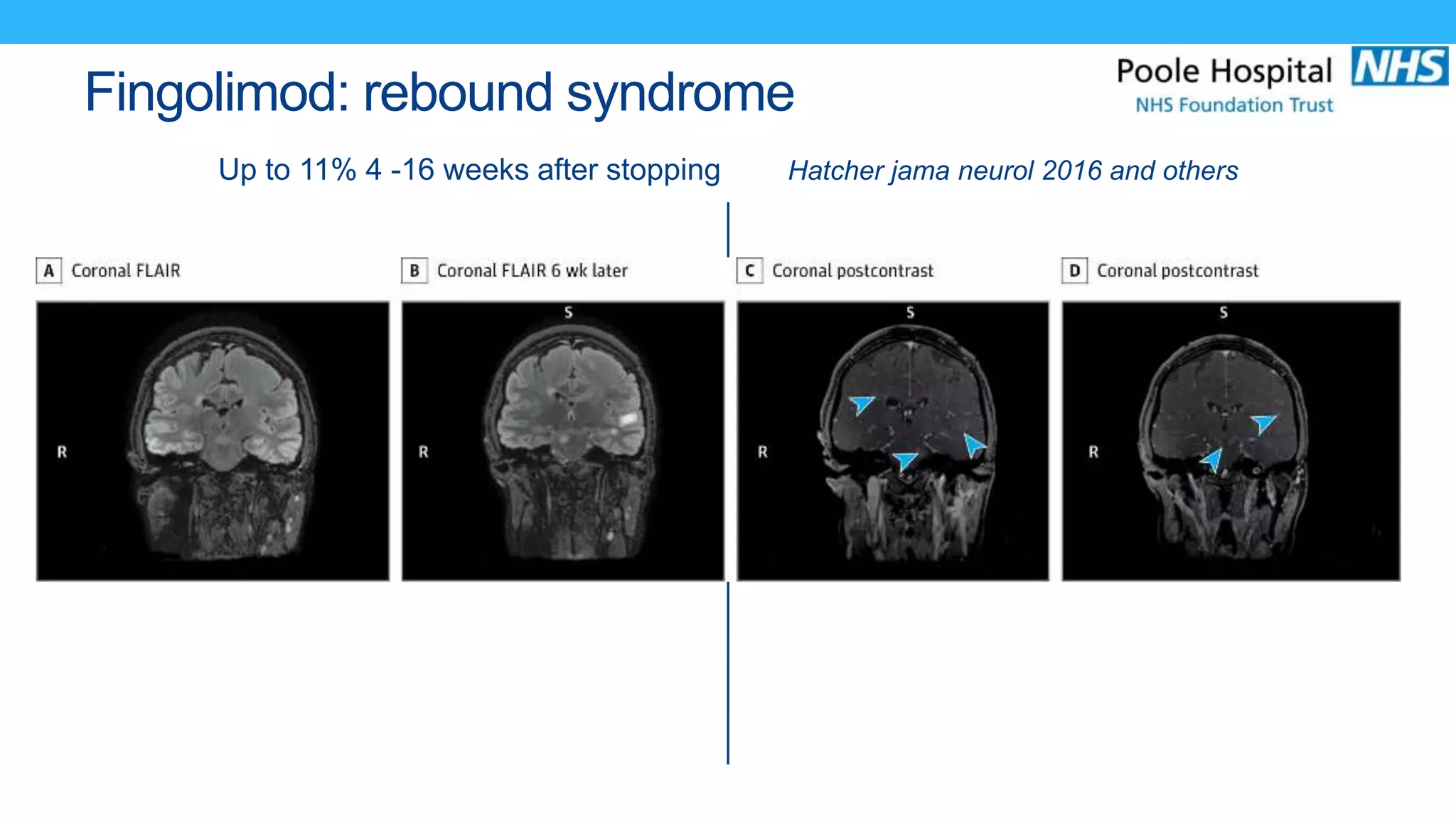











This document discusses guidelines for stopping disease-modifying therapies (DMTs) in multiple sclerosis (MS) patients. It notes that the decision to stop should consider factors like type of MS, disability level, duration of remission, and age. Older patients and those with longer remission periods are less likely to see returns of disease activity after stopping. It also warns that certain DMTs like natalizumab have higher risks of rebound disease activity. The document advocates discussing potential DMT stops before starting treatment and promoting education to help patients make informed decisions.