Downloaded 31 times

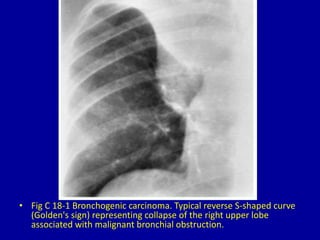
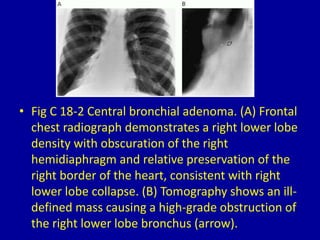
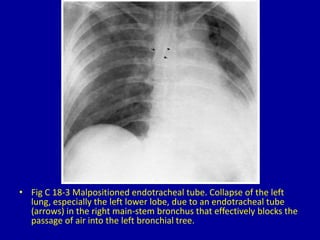
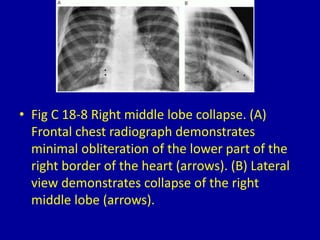
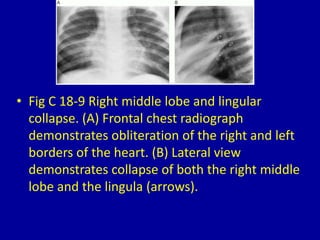
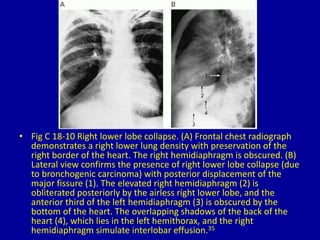




The document discusses lobar or segmental lung collapse seen on chest radiographs and CT scans. It provides 11 figures showing examples of various types of lobar collapse, including collapse of the right or left upper, middle, lower lobes. Common causes of lobar collapse presented are bronchogenic carcinoma, endotracheal tube malposition, mucous plugs, and central bronchial adenomas. Radiographic findings of each type of collapse such as obscuration of vascular structures and fissure lines are described.












































![Imaging in opaqe hemithorax [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/imaginginopaqehemithoraxautosaved-161030071708-thumbnail.jpg?width=640&height=640&fit=bounds)










































