Downloaded 11 times
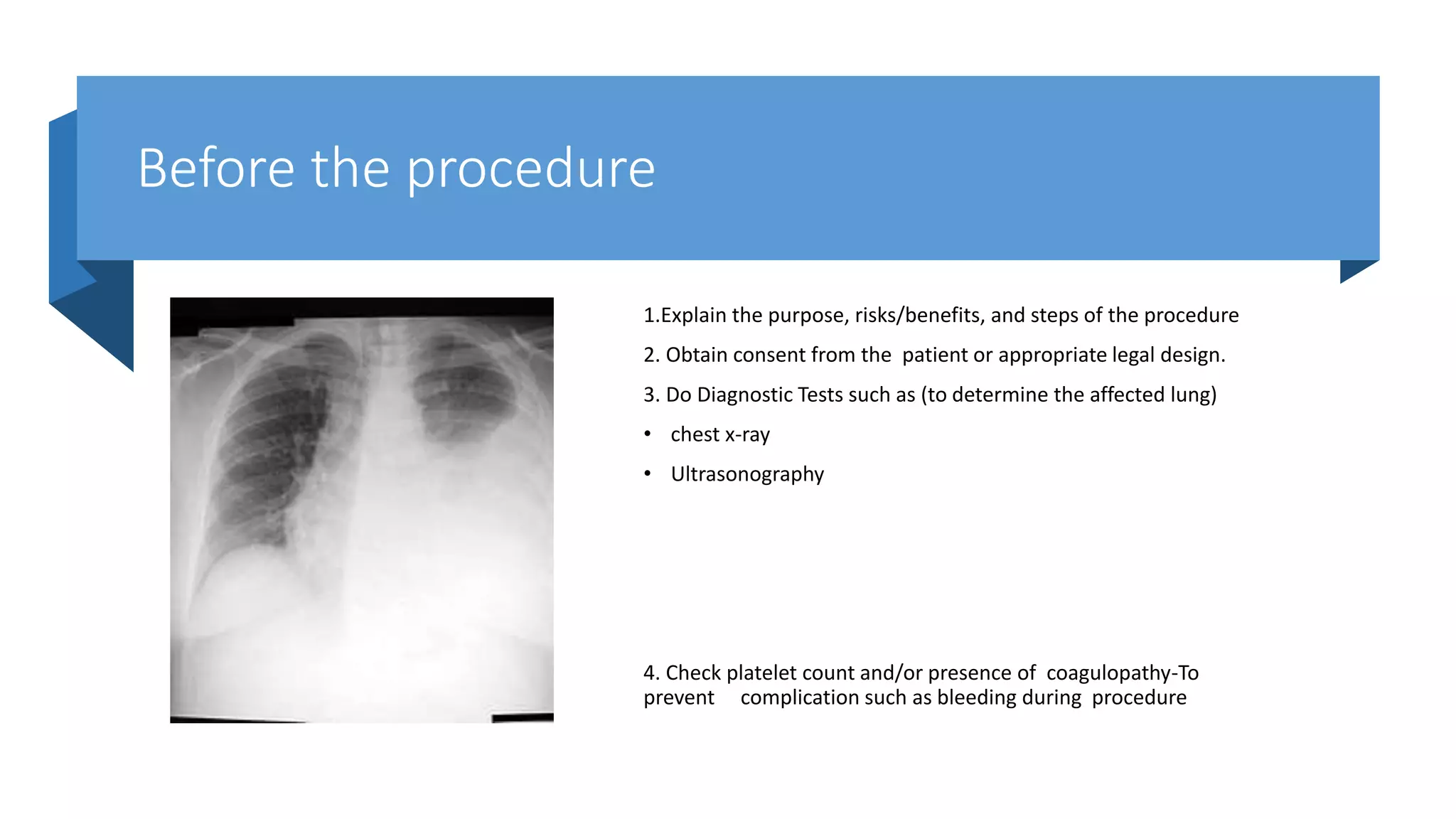
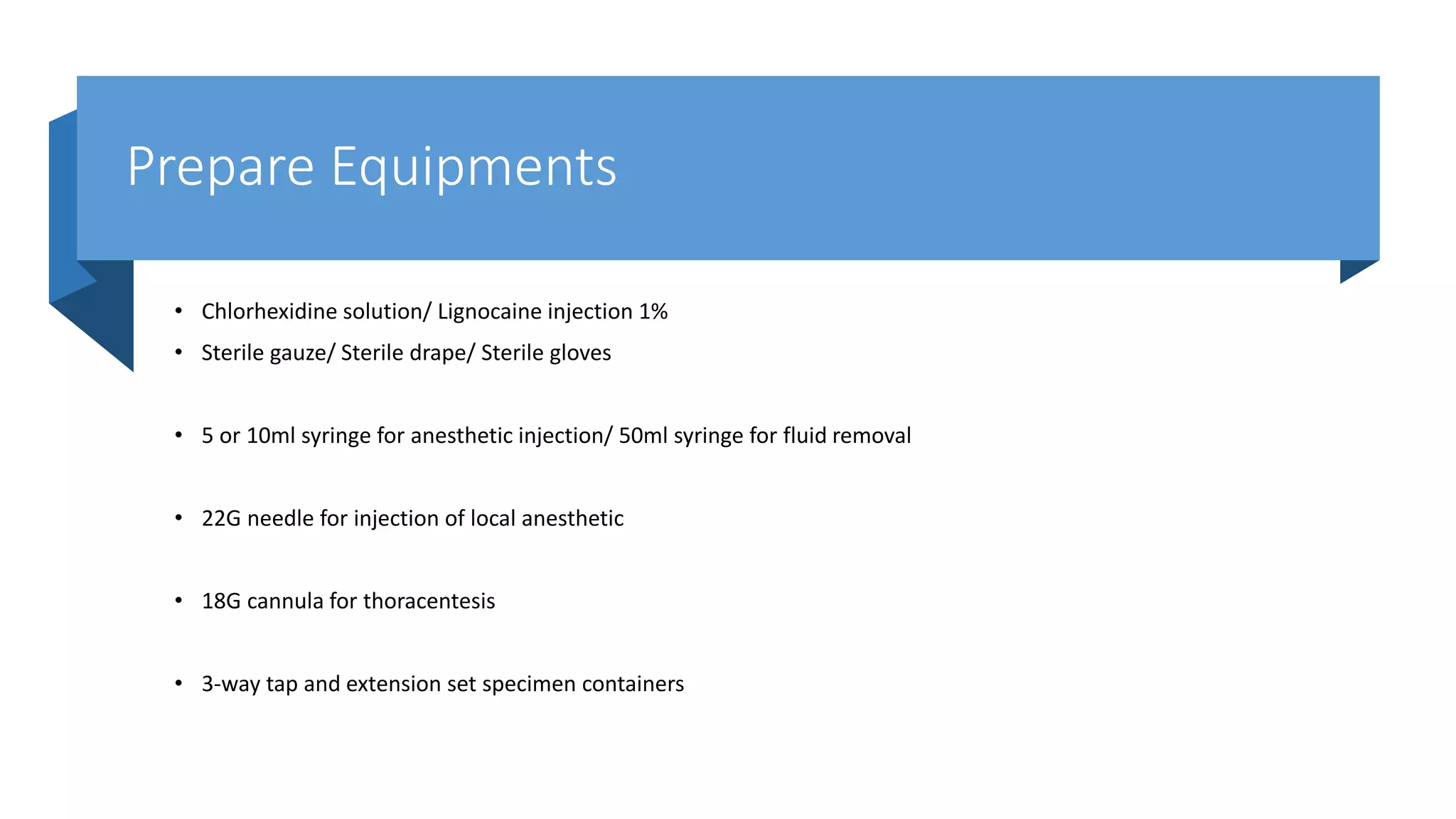
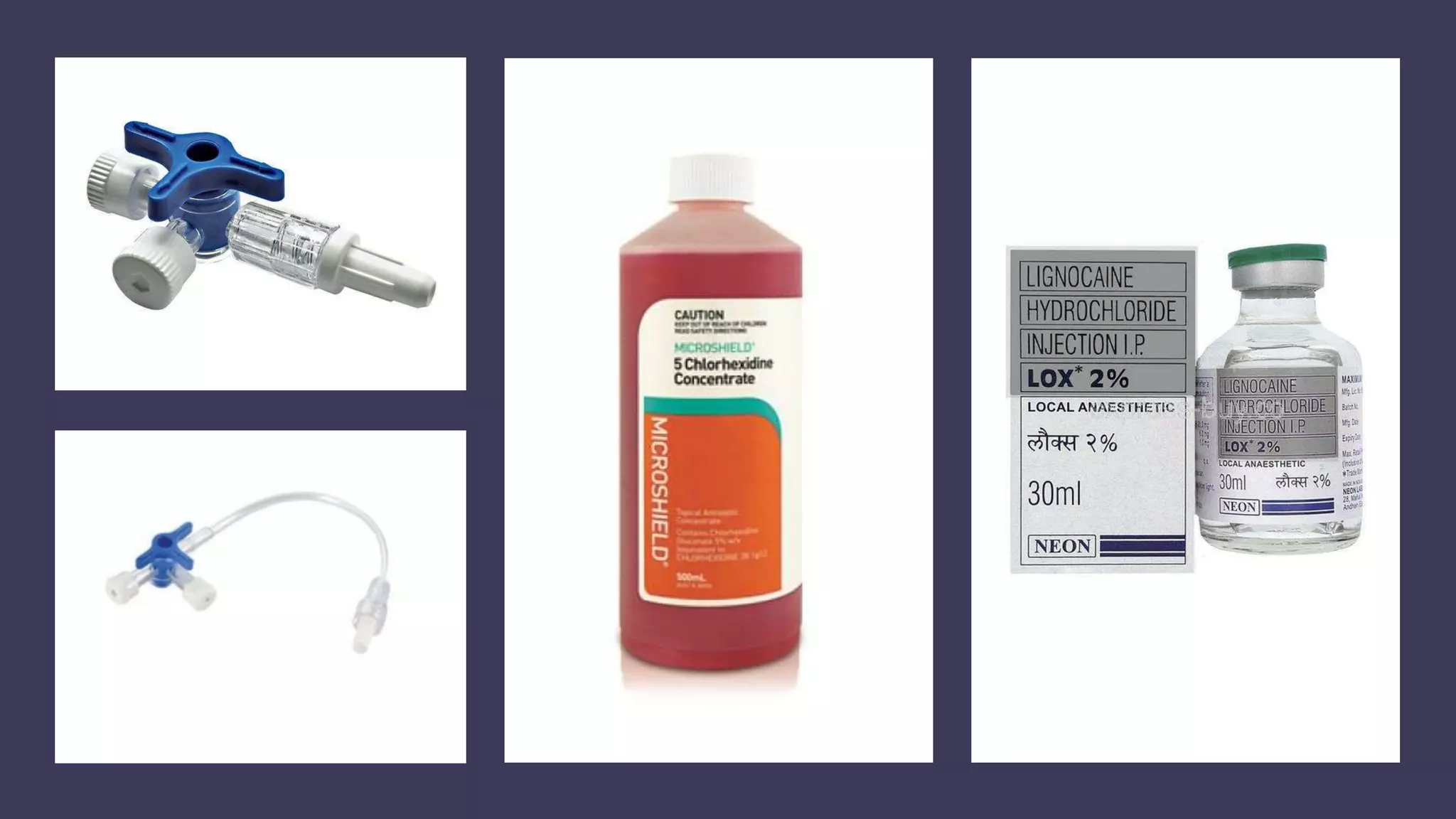

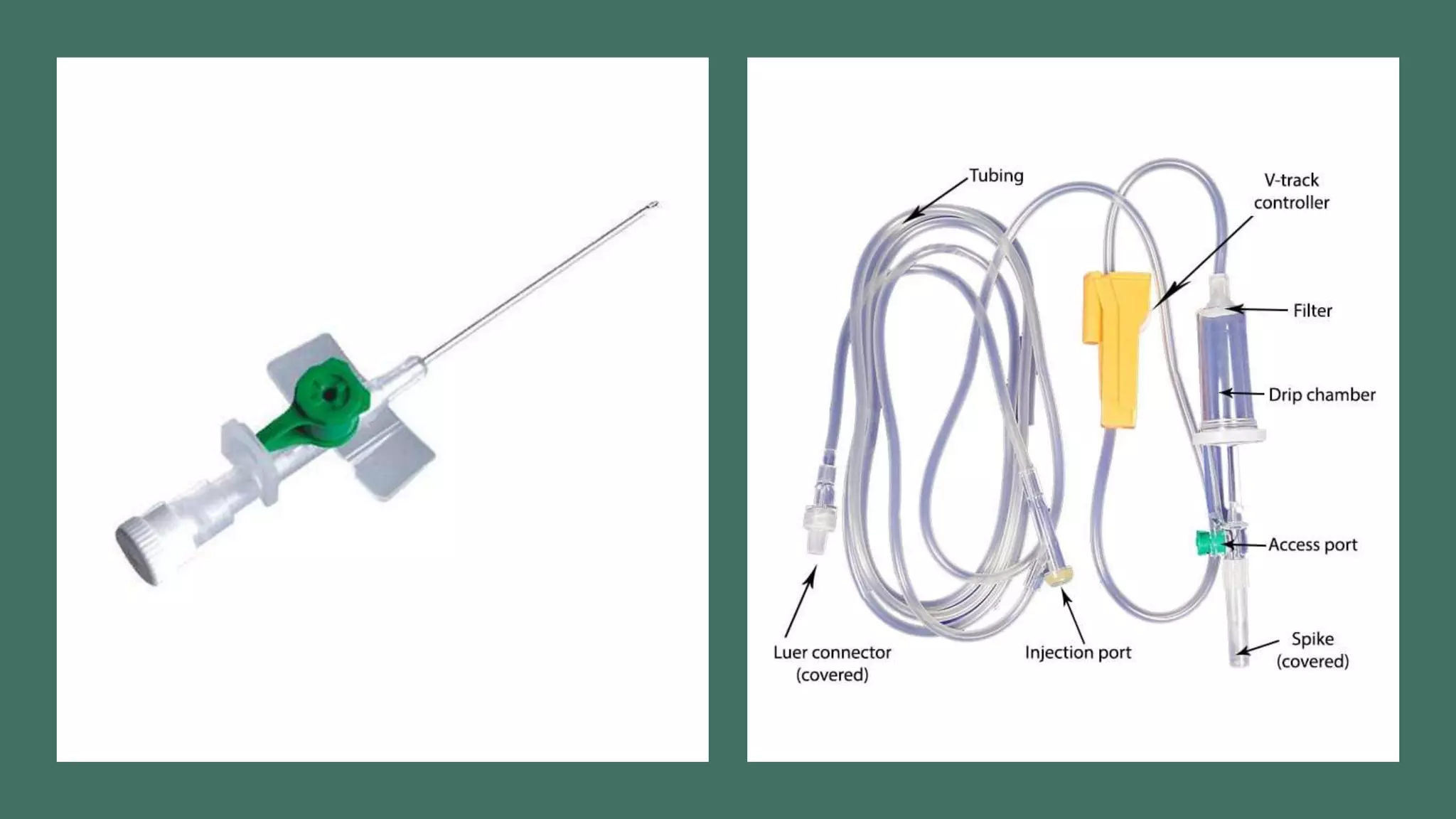


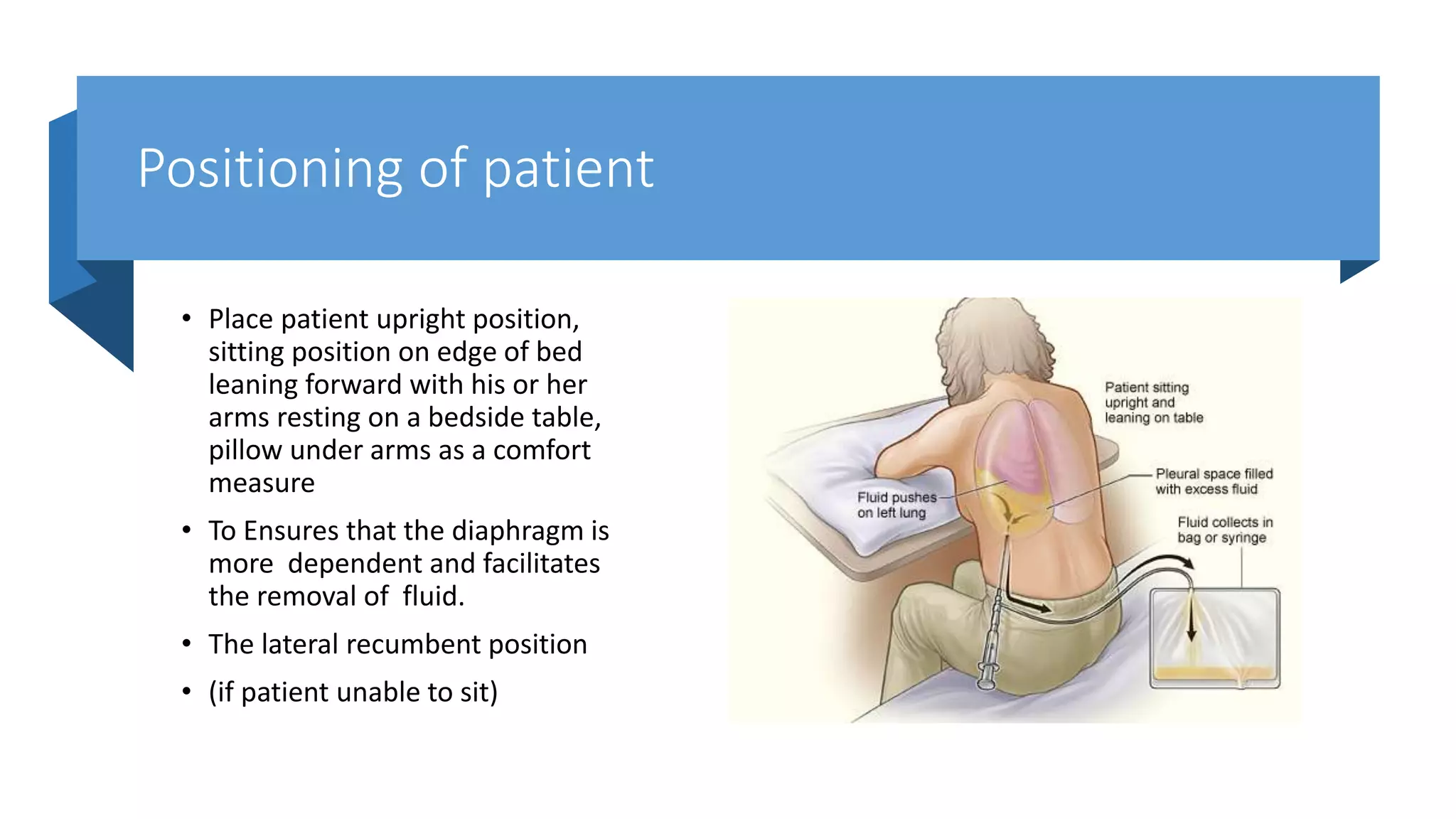






This document provides instructions for performing a thoracentesis procedure. It describes the indications, contraindications, necessary equipment, patient positioning, steps of the procedure, monitoring during the procedure, post-procedure care, potential complications, and instructions for abdominal paracentesis. The key steps are: administering local anesthesia, inserting a cannula or needle into the pleural space, draining pleural fluid for diagnostic testing or therapeutic relief of symptoms, and monitoring for complications such as pneumothorax after the procedure.






![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)




























































