



























Abdominal paracentesis is a medical procedure used to remove peritoneal fluid from the abdominal cavity, often to relieve pressure or for diagnostic purposes related to diseases like liver cirrhosis and certain cancers. It involves careful aseptic technique, patient positioning, and monitoring to prevent complications such as infection or fluid imbalance. Post-procedure care includes sealing the puncture site, monitoring vital signs, and managing any pain or complications.
Introduction to abdominal paracentesis and its significance in nursing.
Abdominal paracentesis defined as needle insertion into the peritoneal space for fluid removal.
Relieves pressure on organs, aids diagnosis, drains exudates, and prepares for procedures.
Determining diagnoses like ascites, and treating discomfort & serious conditions.
Common causes of ascites: cirrhosis, portal hypertension, infections, cancer, organ failure.
Symptoms such as abdominal pain, growing belly, and shortness of breath indicating ascites.
Precautions regarding medication before paracentesis and contraindications for the procedure.
Aseptic technique, patient comfort, fluid withdrawal, and observation during the procedure.
Expected findings in fluid analysis: specific gravity, counts, and protein concentrations.
Essential checks including doctor’s orders, patient condition, and preparation for paracentesis.
Patient consent, skin preparation, privacy, and environmental setup before paracentesis.
Details on site selection to avoid injuries and proper positioning of the patient for paracentesis.
Time taken for paracentesis ranging from 20 to 45 minutes, depending on fluid removal.
Typical volumes of fluid removed: approximately 25 ml for tests, up to 5 liters for relief.
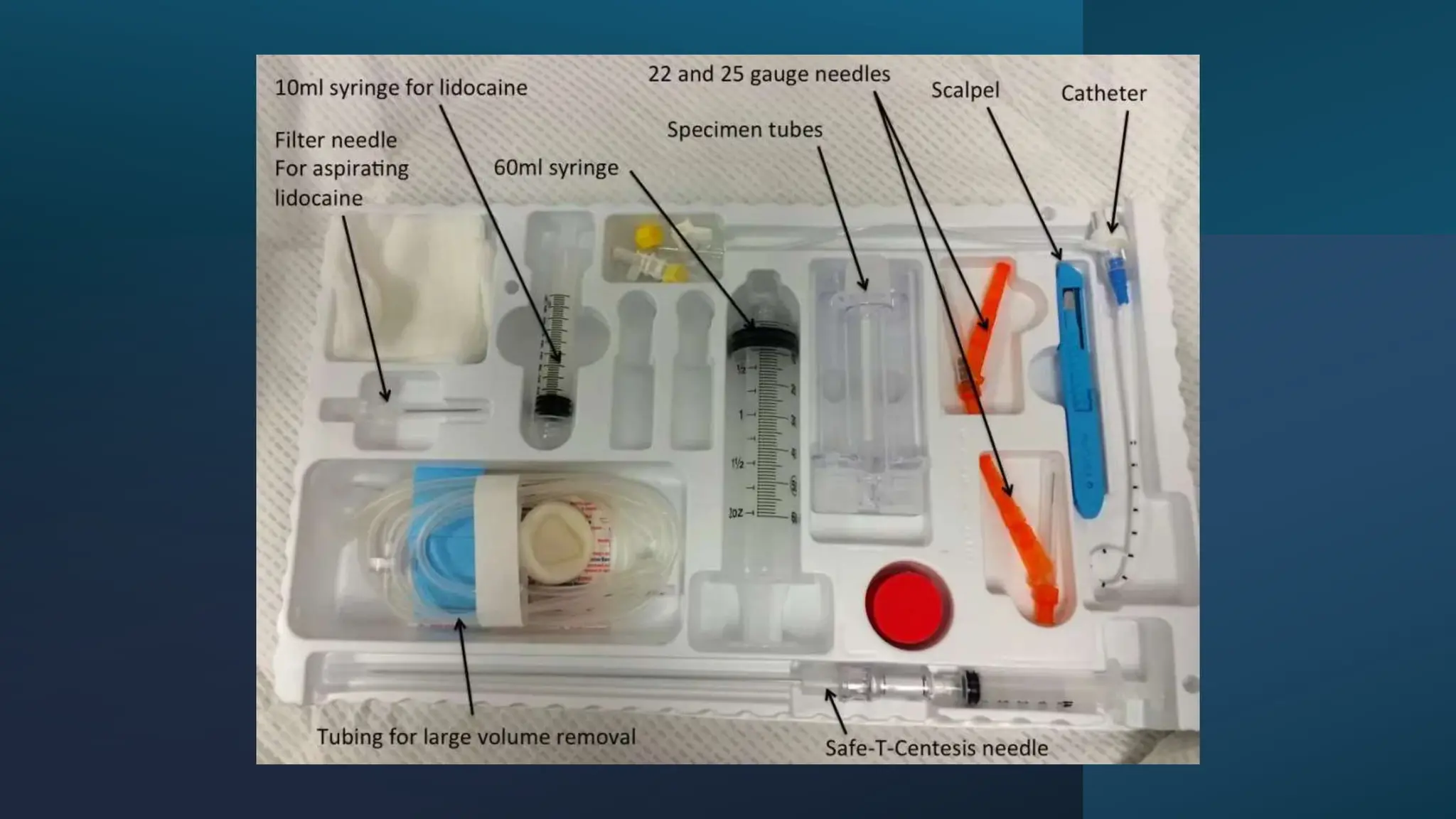
Necessary sterile and unsterile equipment for conducting the paracentesis procedure.
Detailed steps during paracentesis including hand hygiene, patient positioning, and fluid collection.
Post-care steps including applying binders, monitoring, recording, and handling specimens.
Complications like hepatic coma, peritonitis, and fluid dynamics after significant fluid removal.
A clinical example illustrating 7 liters of ascitic fluid drained via paracentesis.
Nurses' role in explaining procedures, educating patients about disease, and lifestyle changes.
Nursing assessments include symptom tracking, determining causes, and monitoring fluid intake.
Techniques to detect ascites: bulging flanks, shifting dullness, and fluid wave examination.
Strategies for managing fluid retention and ensuring risk factors are addressed.
Managing causes of ascites, fluid draining techniques, surgical options, and antibiotic needs.
Key aspects include weight monitoring, alcohol abstinence, NSAIDs caution, and safe practices.
Importance of nursing care plans in ascending interventions and prioritizing patient care.
Sample care plans for ascites addressing fluid volume, nutrition, breathing patterns, and infection.
Closing remarks and gratitude for the participation in the abdominal paracentesis discussion.