Downloaded 1,614 times
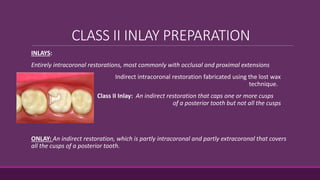










This document provides guidelines for preparing class II inlay restorations. It describes initial procedures like evaluating occlusion and administering anesthesia. It discusses preparing the occlusal outline, proximal box, bevels, and flares. Modifications for specific tooth shapes and situations are covered. Preparation variations like slices and flares are explained. Special considerations for abutment teeth and root surface lesions are also summarized. The document provides a thorough overview of class II inlay preparation techniques.






















































































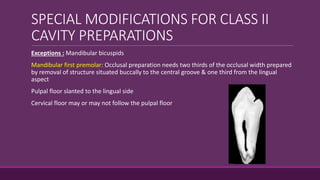
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














