Downloaded 689 times
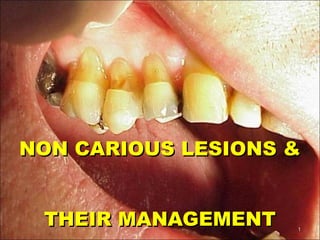














Non-carious lesions can be caused by various factors like attrition, abrasion, abfraction, erosion, and developmental defects. They are managed through treatments like restoration, controlling parafunctional habits, and addressing underlying causes. Localized enamel hypoplasia can result in pits and defects from interruptions during enamel formation, while hypocalcification makes enamel softer and more stainable. Management involves restoration, bleaching, or preventing further demineralization.