Downloaded 2,653 times

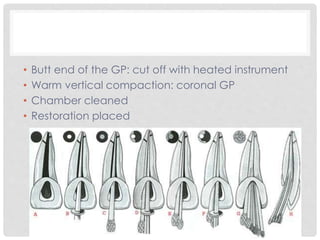

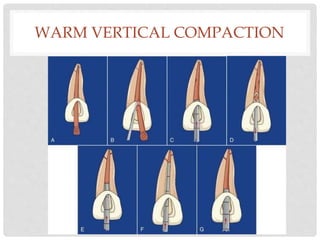

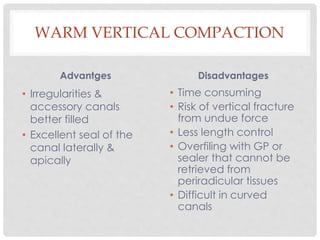

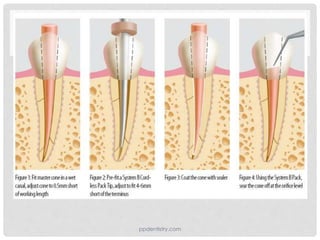
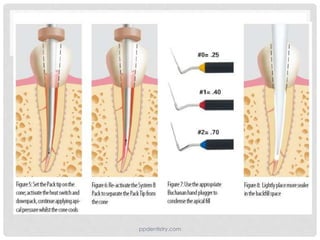
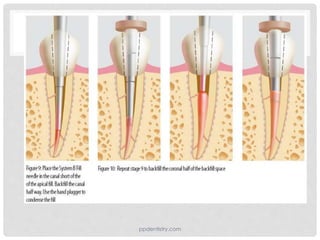




This document discusses various obturation techniques for filling root canals including: 1. Cold lateral compaction, the most widely used technique, involves inserting a master cone coated with sealer followed by lateral compaction of accessory cones. 2. Warm vertical compaction uses heated pluggers to vertically compact gutta percha that has been softened with heat. 3. Carrier-based techniques like Thermafil involve heating and inserting a gutta percha coated metal core carrier into the canal. The document provides details on how to perform each technique and their advantages and disadvantages. A variety of materials can be used for obturation including gutta percha, resins, and single cone techniques.















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

