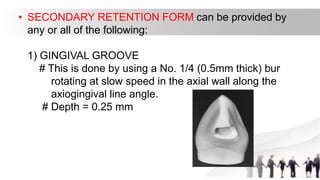
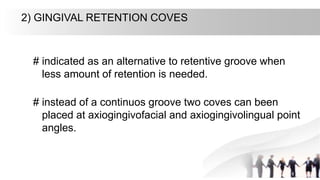
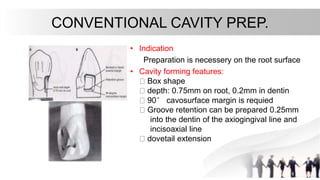
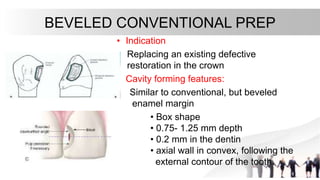
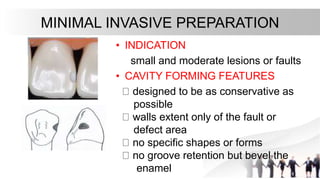
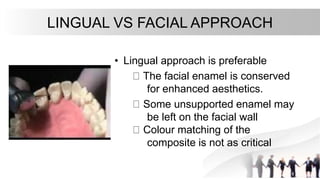
This document discusses Class III cavity preparations, which involve the proximal surfaces of anterior teeth. It defines Class III cavities and compares amalgam versus composite restorations. It provides indications and contraindications for different types of Class III preps and describes the steps for outlining, forming resistance/retention features, finishing walls, and lingual versus facial approaches.