

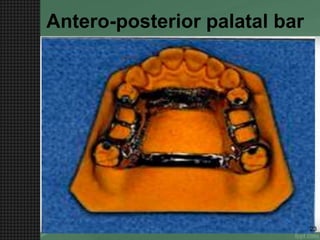


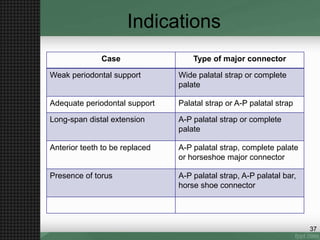
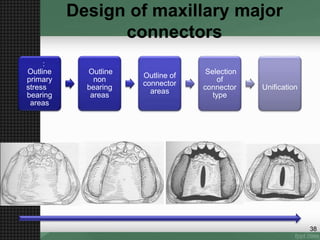


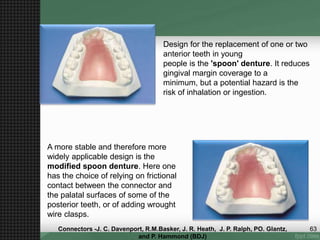
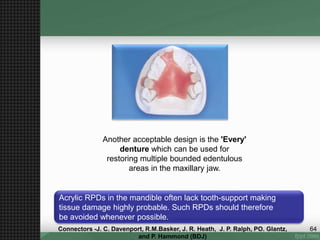
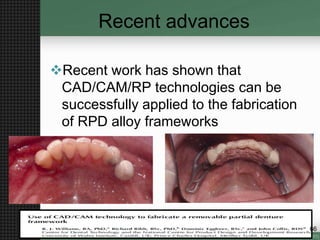
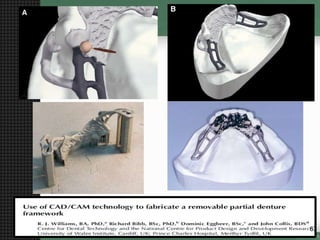
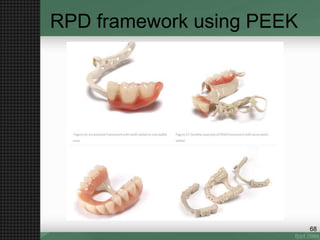


The document discusses major connectors used in removable partial dentures, detailing their roles, types, and design requirements for both maxillary and mandibular connectors. It covers various types, including palatal straps, lingual bars, and their indications, advantages, and disadvantages. Recent advancements, such as CAD/CAM technologies in fabrication, are also mentioned alongside a conclusion and references.


















































































