Download as PDF, PPTX
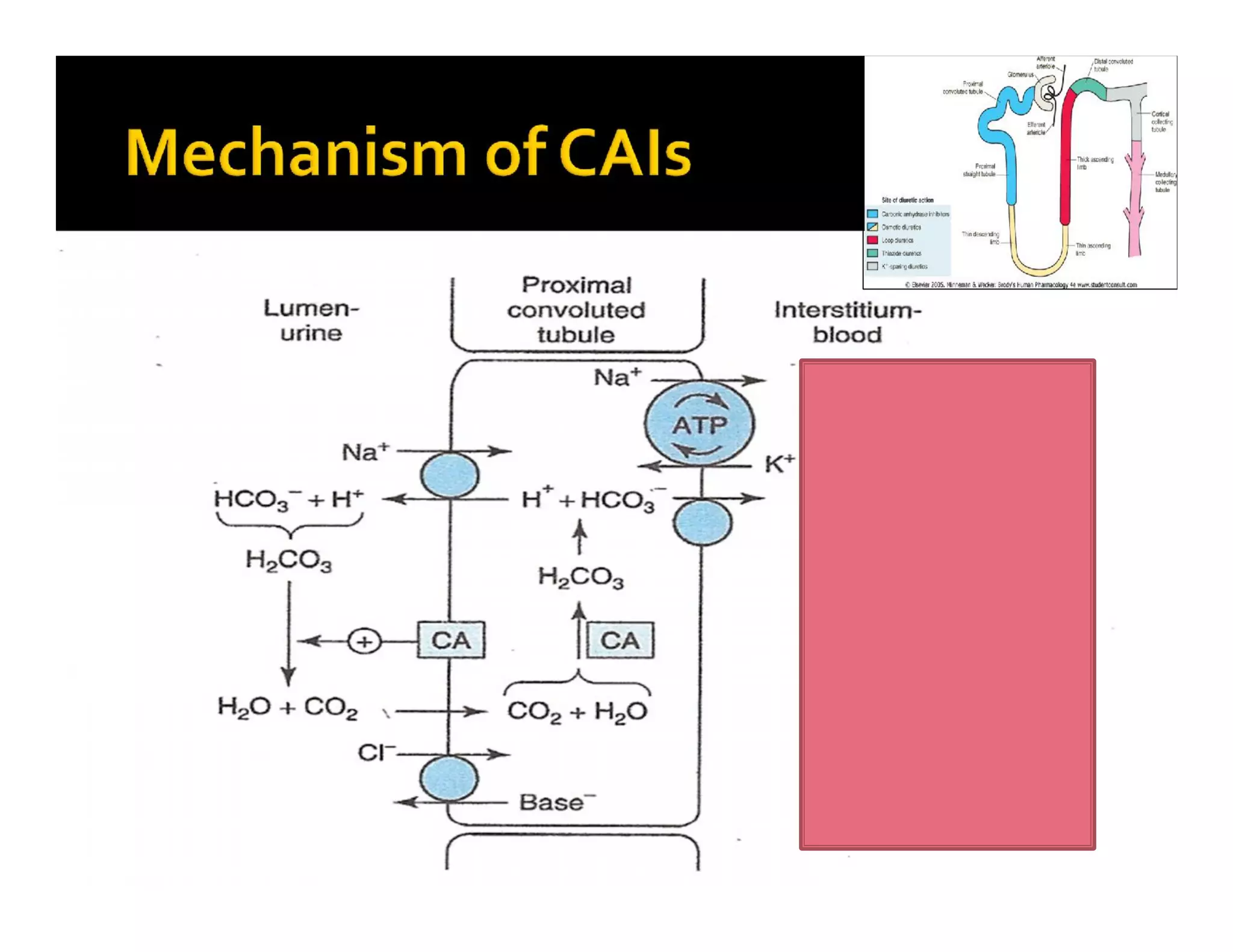
![inhibits carbonic anhydrase in
renal proximal tubule cells
carbonic anhydrase catalyzes
formation of HCO3- and H+ from
H2O and CO2
inhibition of carbonic anhydrase
decreases [H+] in tubule lumen
less H+ for Na+/H+ exchange
increased lumen Na+, increased
H2O retention](https://image.slidesharecdn.com/classdiuretics-140805005429-phpapp01/75/Class-diuretics-24-2048.jpg)
![ Used to treat chronic open-angle glaucoma
aqueous humor has high [HCO3-]
Acute mountain sickness decrease CSF formation
and by decreasing pH
Metabolic alkalosis they can produce
hyperchloremic acidosis
Sometimes in epilepsy decreasing the pH
Mostly used in combination with other diuretics in
resistant patients
Alkalinisation of urine](https://image.slidesharecdn.com/classdiuretics-140805005429-phpapp01/75/Class-diuretics-25-2048.jpg)


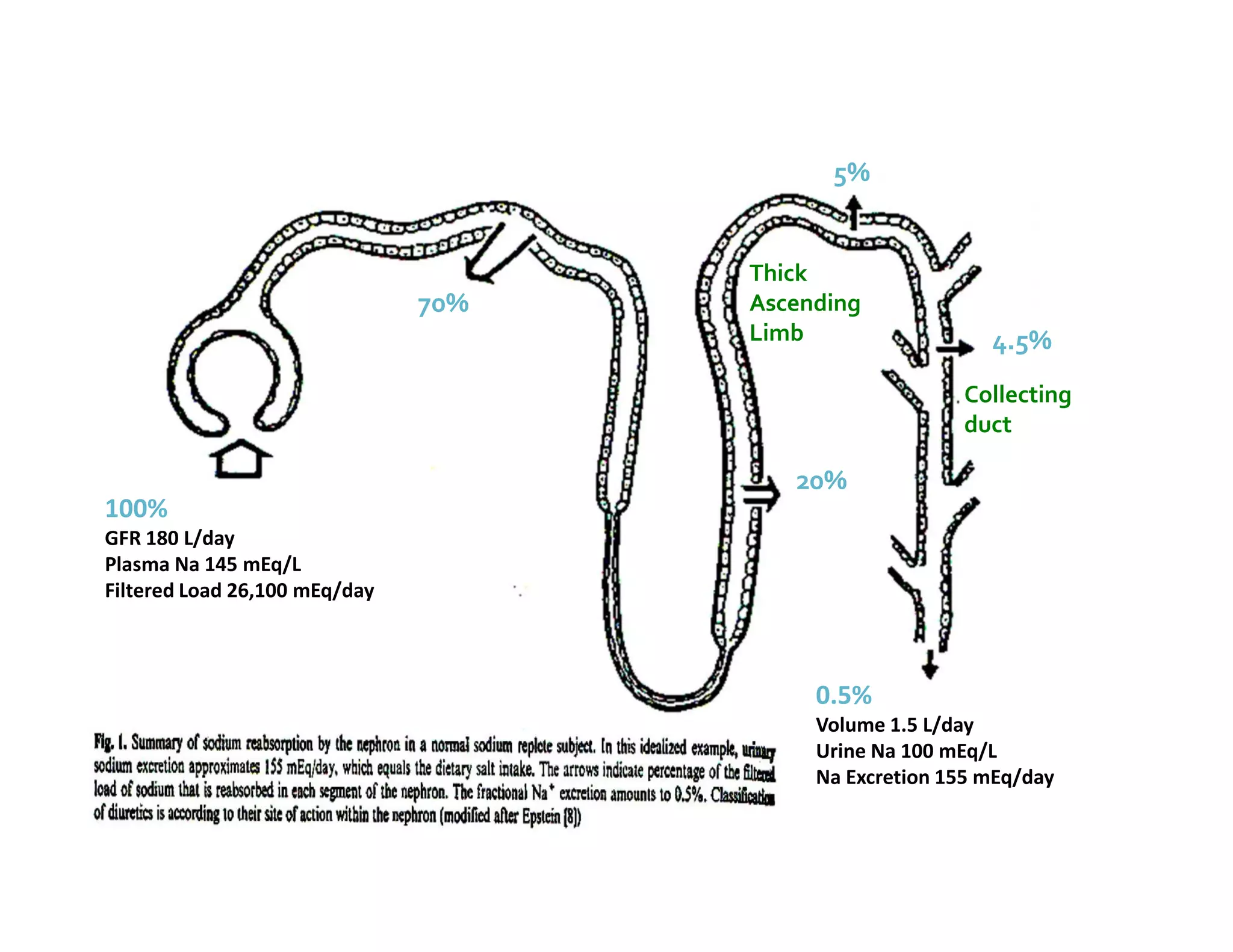
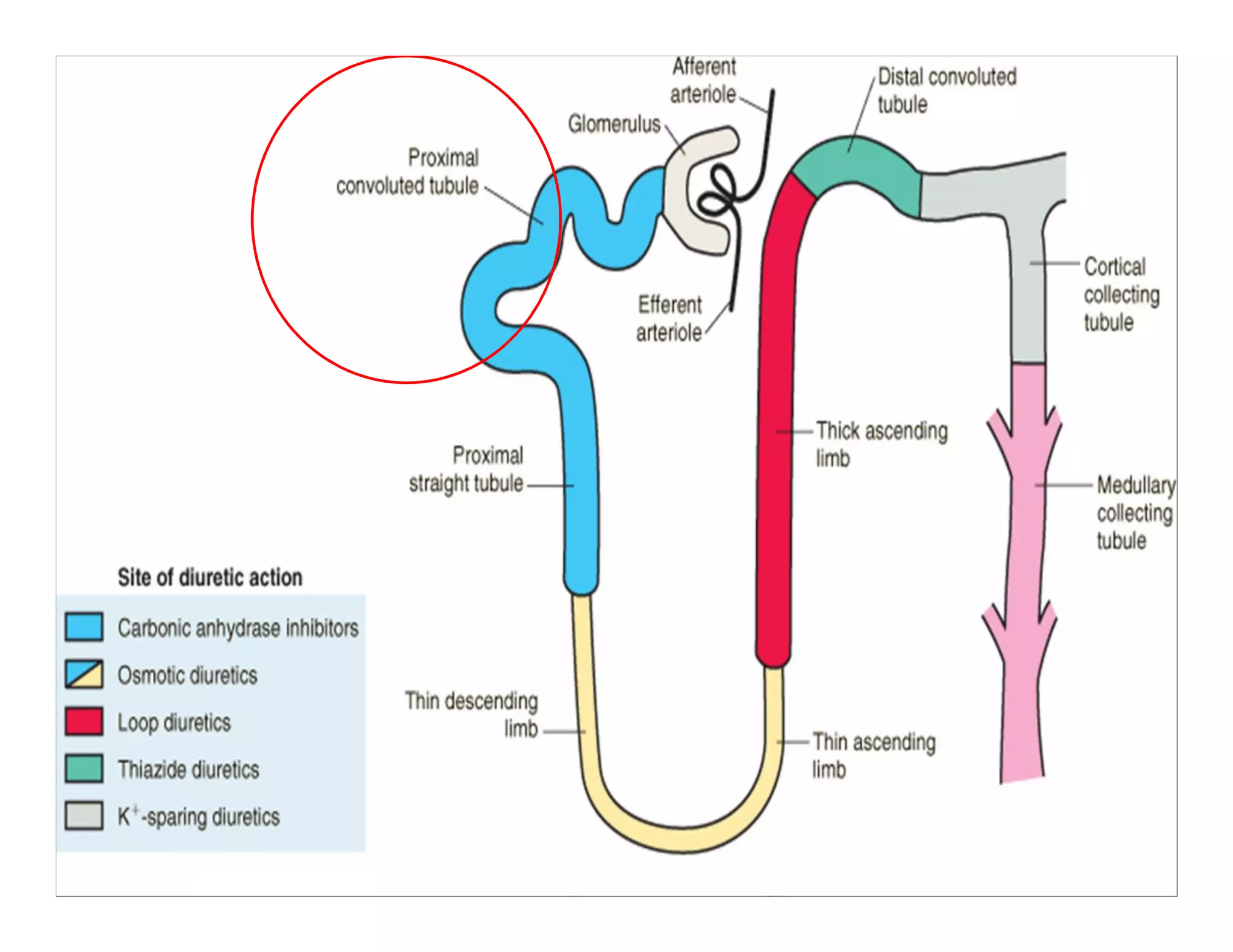
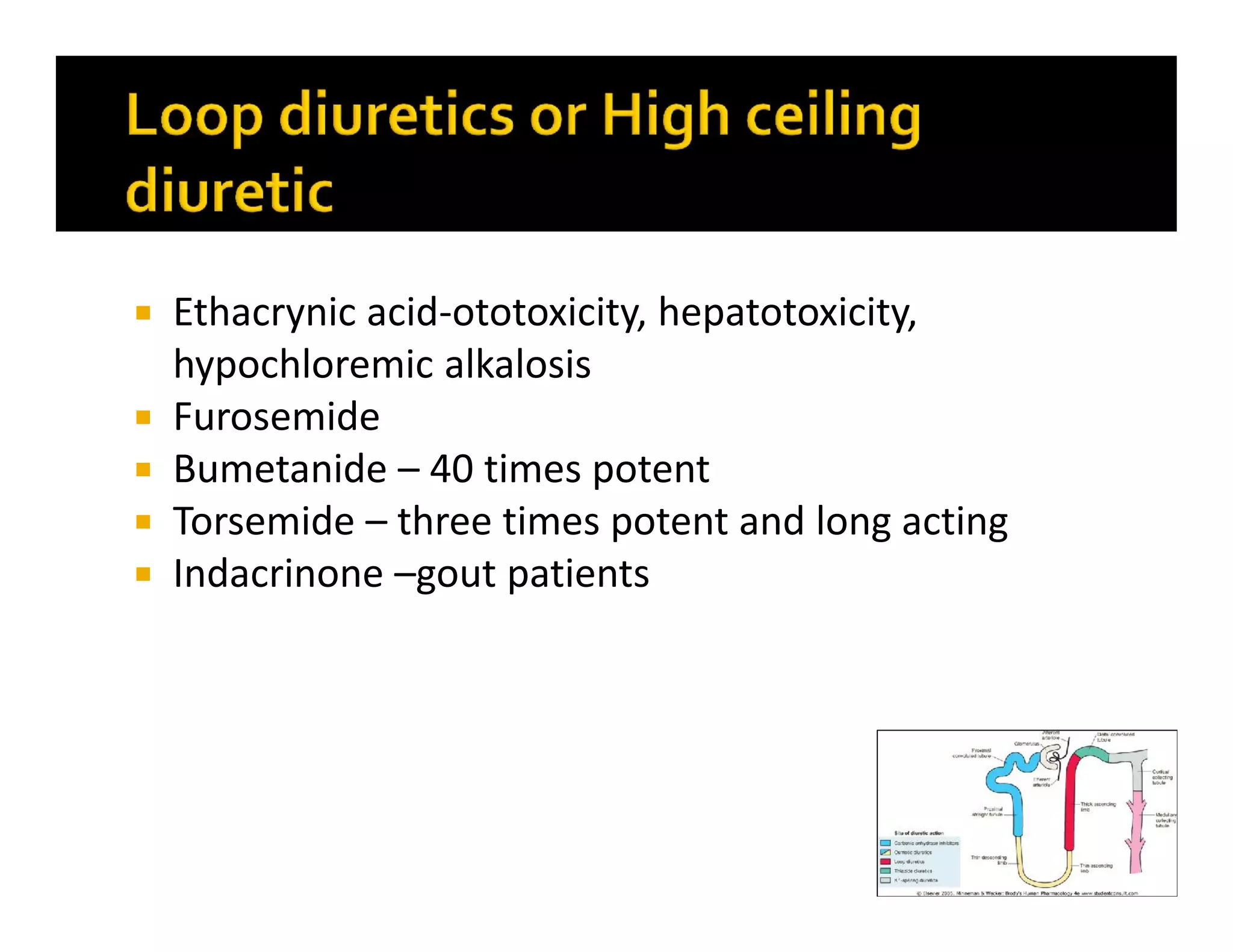
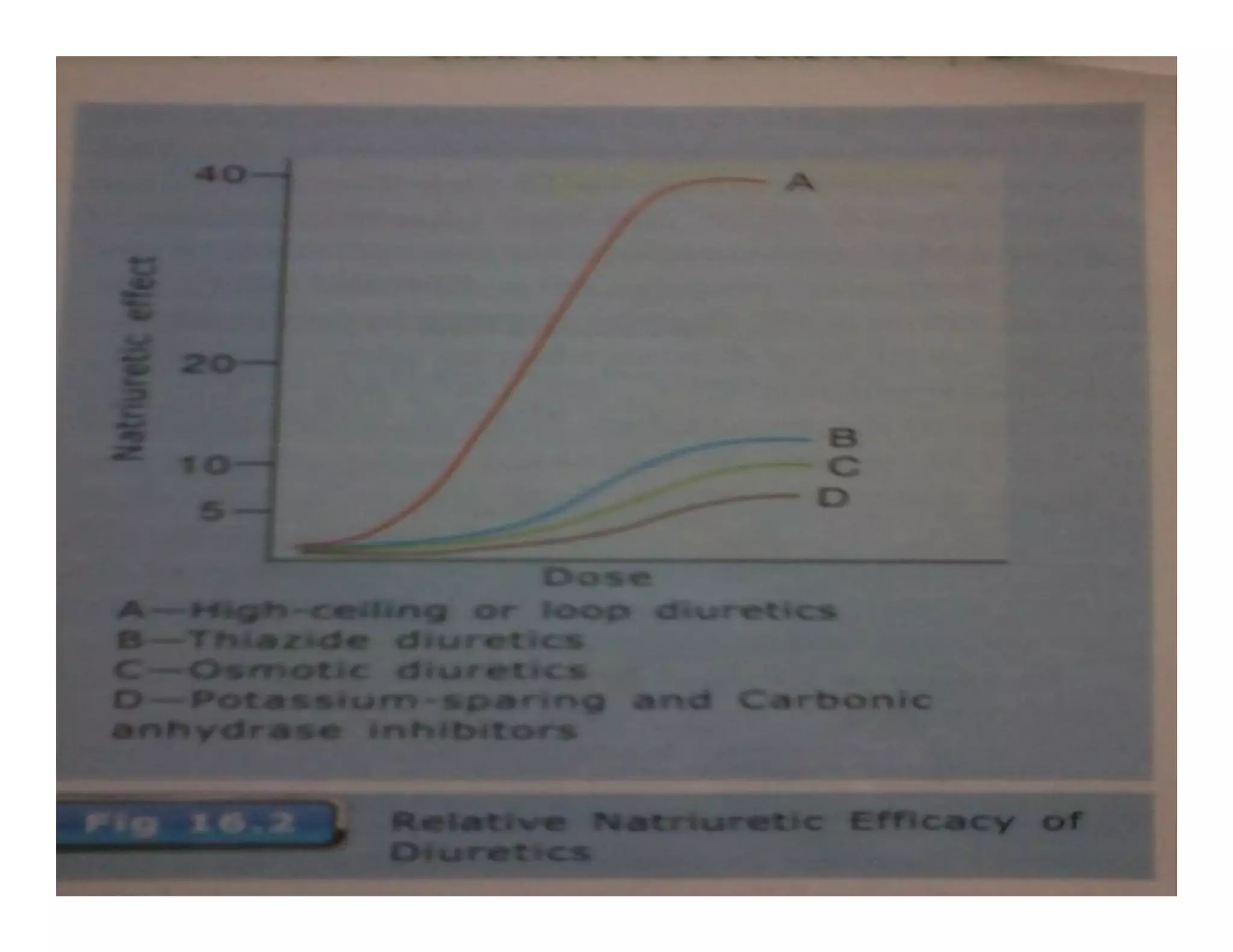
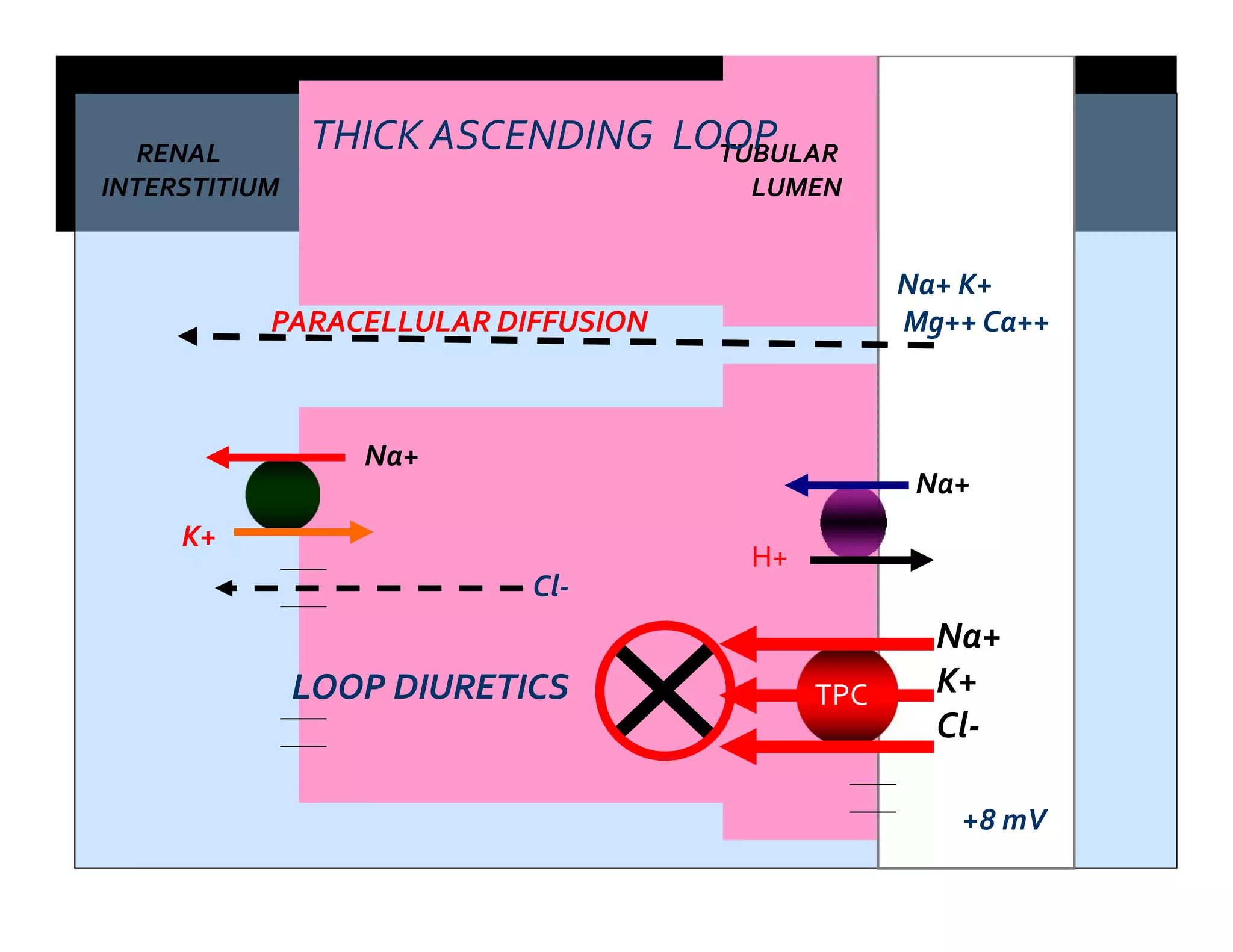
This document provides information on diuretic drugs, including their mechanisms and sites of action, indications for use, and adverse effects. It discusses loop diuretics like furosemide and bumetanide that act in the thick ascending loop of Henle, thiazide diuretics like hydrochlorothiazide that act in the distal tubule, and potassium-sparing diuretics like amiloride and spironolactone that act in the collecting ducts. It also covers carbonic anhydrase inhibitors and osmotic diuretics. Non-diuretic uses and combinations with other drugs are mentioned. Resistance, interactions, and specific adverse effects are summarized for each drug class.











































































































