Downloaded 2,206 times





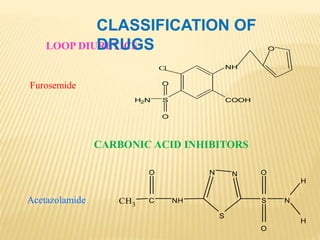








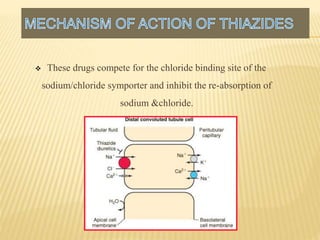




















The document presents an overview of diuretics, including their classification, mechanisms of action, and therapeutic uses, particularly in conditions like hypertension and heart failure. It details various diuretic types, including loop diuretics, thiazides, and potassium-sparing diuretics, along with their pharmacological effects and side effects. Additionally, it acknowledges sources of information and expresses gratitude to the guide and committee involved in the research presentation.









































































![ANTIBIOTICS[PENICILLINS] MEDICINAL CHEMISTRY BY RAVISANKAR](https://cdn.slidesharecdn.com/ss_thumbnails/penicillin-1-ppt-new-130616074411-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















