Downloaded 221 times
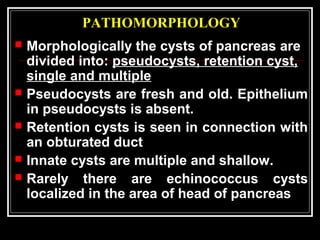
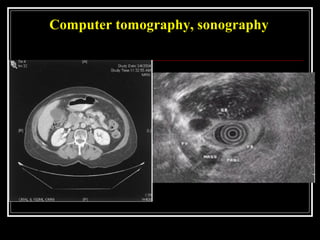
![TESTS FOR CHRONIC PANCREATITIS
MEASUREMENT OF PANCREATIC PRODUCTS IN BLOOD
I A Enzymes
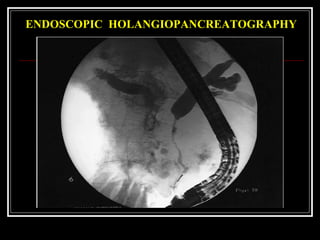
B Pancreatic polypeptide
MEASUREMENT OF PANCREATIC EXOCRINE SECRETION
II A Direct measurements
1 Enzymes
2 Bicarbonate
B Indirect measurement
1 Bentiromide test
2 Schilling test
3 Fecal fat, chymotrypsin, or elastase concentration
4 [14
C]-olein absorption
IMAGING TECHNIQUES
III A Plain film radiography of abdomen
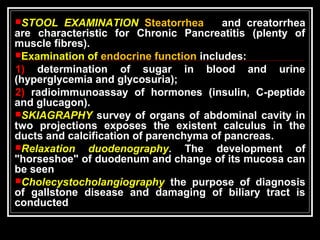
B Ultrasonography
C Computed tomography
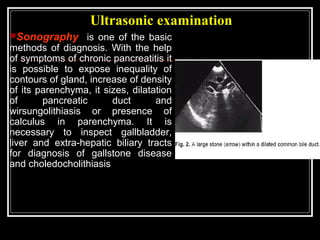
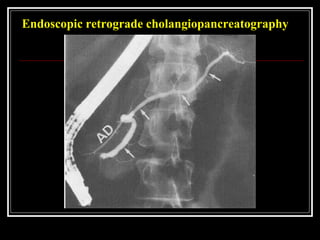
D Endoscopic retrograde cholangiopancreatography
E Magnetic resonance cholangiopancreatography
F Endoscopic ultrasonography
G Relaxation duodenogram](https://image.slidesharecdn.com/lecturechronicpancreatitis2-160124125826/85/Lecture-chronic-pancreatitis-20-320.jpg)


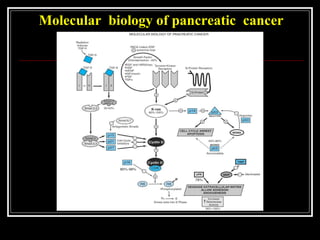


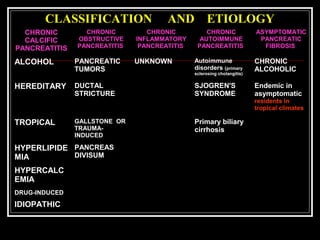
This document discusses chronic pancreatitis, including its causes, pathogenesis, classification, clinical presentation, diagnostic evaluation, complications, and surgical and non-surgical management. Some key points include: - Gallstone disease is the most common cause, accounting for 70% of cases. Other causes include alcoholism, trauma, genetic factors. - Pathogenesis involves reflux of infected bile or duodenal contents into the pancreatic ducts, causing inflammation and activation of pancreatic enzymes. - Classification is based on etiology, presence of pancreatic duct obstruction, and clinical features such as pain pattern. - Presentation includes recurrent upper abdominal pain, weight loss from malabsorption, and endocrine and exocrine pancreatic insufficiency



































































