Downloaded 719 times

![References
• Advances in Wound Healing: A Review of Current Wound Healing Products
Patrick Murphy and Gregory R. D. Evans,Aesthetic and Plastic Surgery
Institute, University of California Irvine Medical Center, 200 S. Manchester
Avenue, Suite 650, Orange, CA 92868, USA
• M. Trop, M. Novak, S. Rodl, B. Hellbom, W. Kroell, and W. Goessler, “Silver-
coated dressing acticoat caused raised liver enzymes and argyria-like symptoms
in burn patient,” Journal of Trauma, vol. 60, no. 3, pp. 648–652, 2006.
• E. K. Mooney, C. Lippitt, and J. Friedman, “Silver dressings [safety and efficacy
reports],” Plastic and Reconstructive Surgery, vol. 117, no. 2, pp. 666–669, 2006.
• W. Stanford, B. W. Rappole, and C. L. Fox, “Clinical experience with silver
sulfadiazine, a new topical agent for control of pseudomonas infections in
burns,” Journal of Trauma, vol. 9, no. 5, pp. 377–388, 1969.](https://image.slidesharecdn.com/recentadvancesinwoundhealing-150525112158-lva1-app6891/85/Recent-advances-in-wound-healing-63-320.jpg)
![• R. Warriner and R. Burrell, “Infection and the chronic wound: a focus on
silver,” Advances in skin & wound care., vol. 18, pp. 2–12, 2005.
• B. S. Atiyeh, M. Costagliola, S. N. Hayek, and S. A. Dibo, “Effect of silver on
burn wound infection control and healing: review of the literature,” Burns, vol.
33, no. 2, pp. 139–148, 2007.
• R. Khundkar, C. Malic, and T. Burge, “Use of Acticoat dressings in burns: what
is the evidence?” Burns, vol. 36, no. 6, pp. 751–758, 2010.
• Winter GD. Formation of scab and rate of epithelialization of superficial
wounds in the skin of the young domestic pig. Nature. 1962;193:293–4.
• Cho CY, Lo JS. Excision and repair: Dressing the
part. DermatolClin. 1998;16:25–47. [PubMed]](https://image.slidesharecdn.com/recentadvancesinwoundhealing-150525112158-lva1-app6891/85/Recent-advances-in-wound-healing-64-320.jpg)


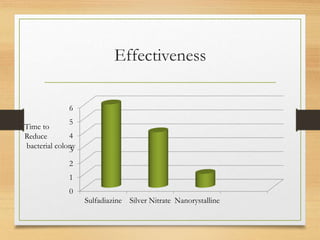
The document discusses recent advances in wound healing, including silver-based dressings, negative pressure therapy, advanced dressings like hydrocolloids and alginates, skin substitutes, growth factors, and hyperbaric oxygen therapy. Silver dressings provide antimicrobial properties and sustained silver ion release. Negative pressure therapy promotes wound healing through macro and micro strain. Advanced dressings maintain a moist wound environment. Skin substitutes and growth factors can accelerate healing.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














