




























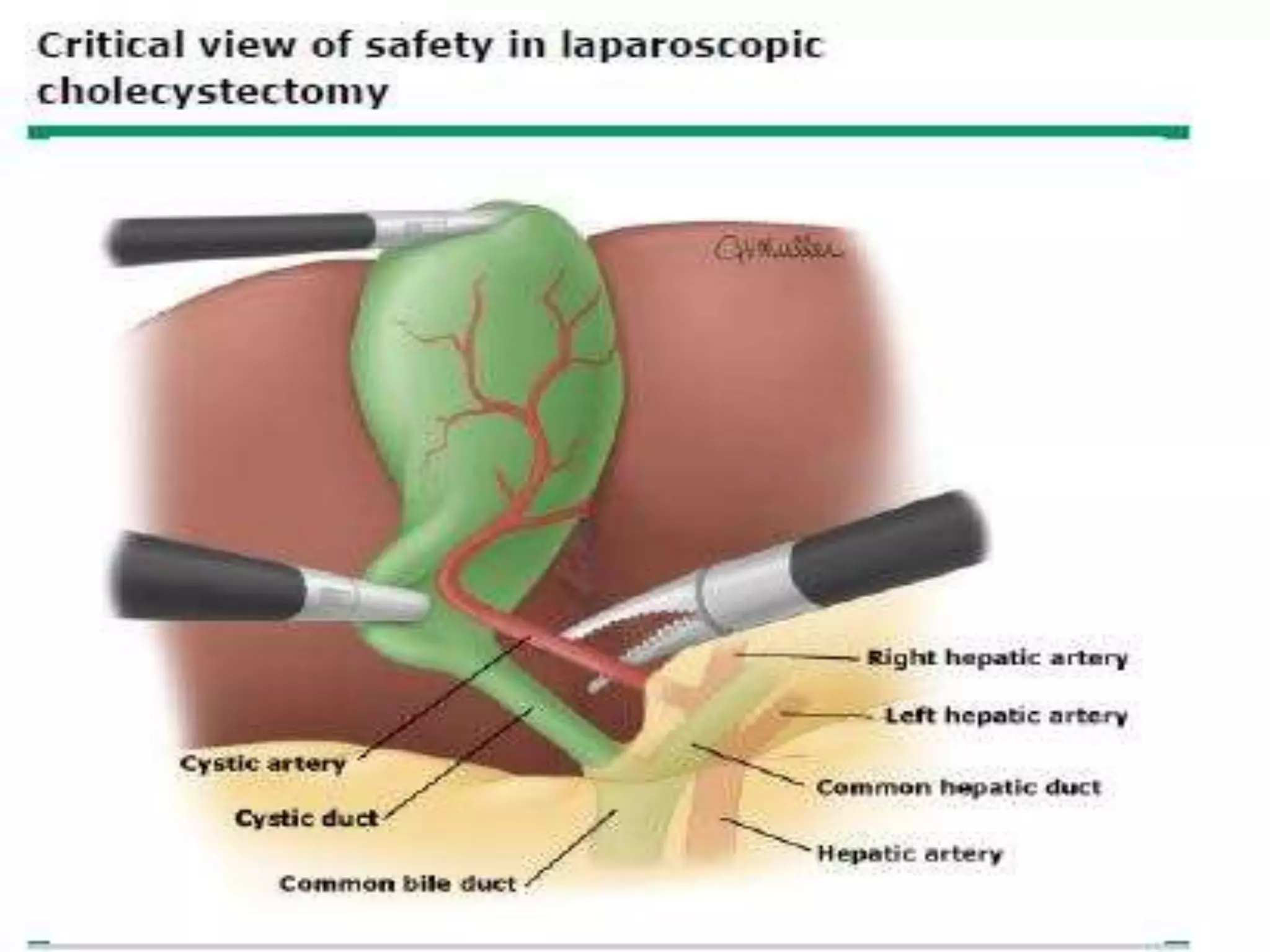































The presentation discusses safe laparoscopic cholecystectomy techniques, emphasizing its advantages such as reduced pain and faster recovery compared to open surgery. Key topics include preoperative preparation, operative techniques, and safety measures like the critical view of safety to minimize bile duct injuries. Various indications, contraindications, and the importance of proper anatomy identification during surgery are also highlighted.























































































