This document discusses subaxial cervical spine injuries, including:
- Assessment and emergency treatment of cervical spine injuries following trauma.
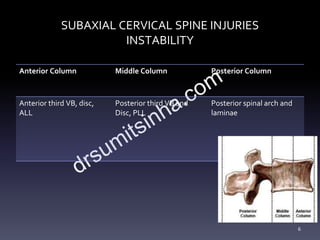
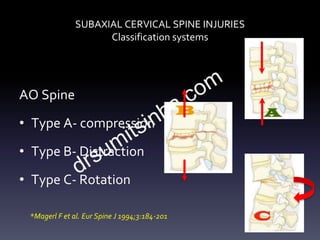
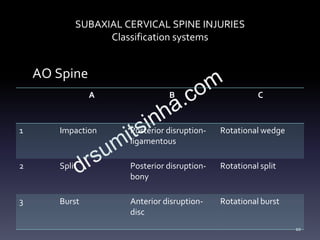
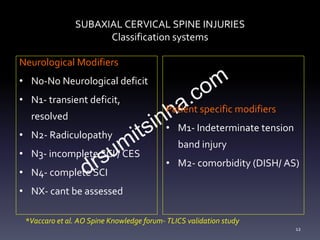
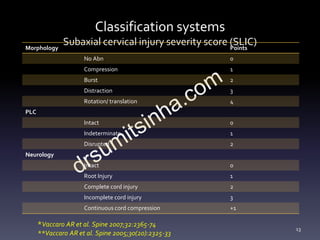
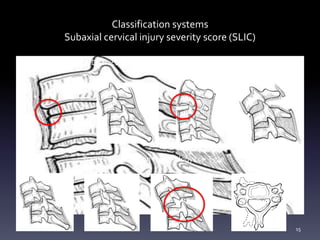
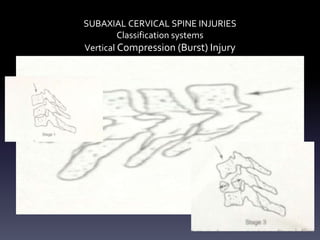
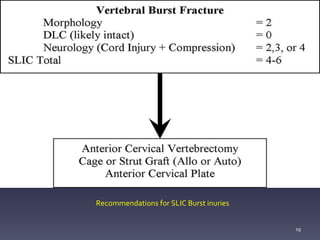
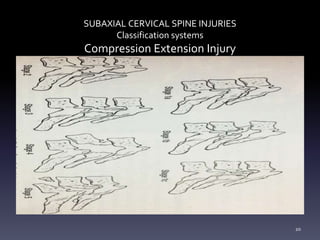
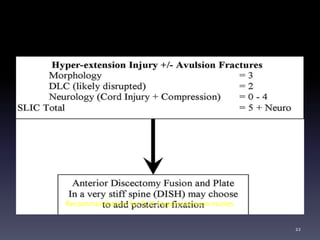
- Classification systems for cervical spine injuries including AO Spine, SLIC, and others which classify injuries based on morphology, neurological status, and stability.
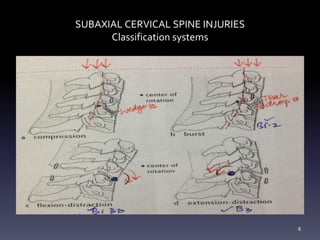
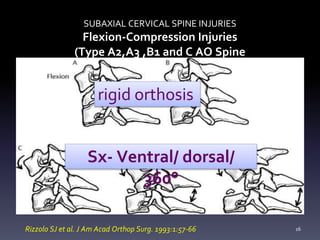
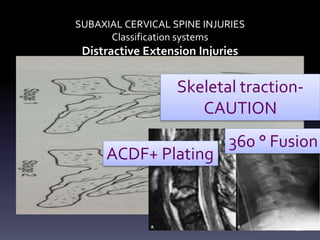
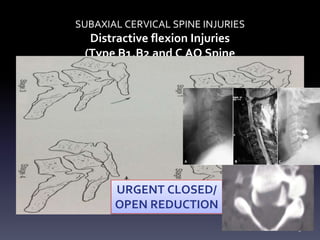
- Types of cervical injuries such as flexion-compression, burst fractures, distraction injuries, and recommendations for treatment and surgery based on classification.
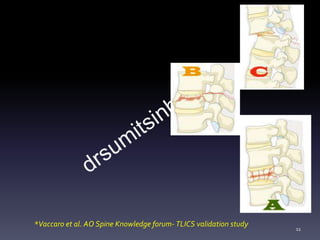
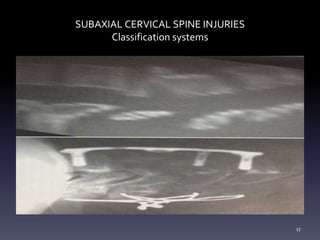
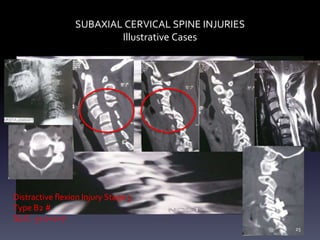
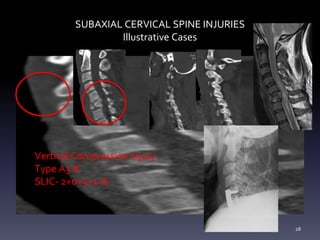
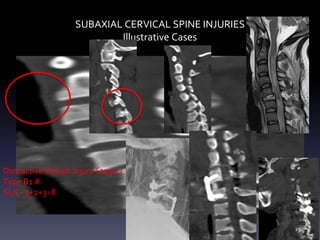
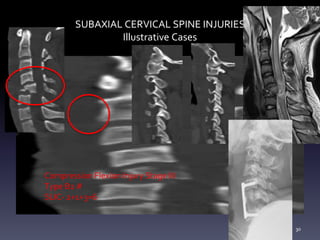
- Illustrative case examples of different cervical injury types classified using AO Spine and SLIC systems along with their treatments.
- Key points about immobilizing the cervical spine, rational use of imaging, importance of stability especially the posterior column, and indications for early surgery.



















































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)








