Downloaded 128 times













![Combination Therapy
• Ipratropium+albuterol (DuoNeb®, generic)
[0.5 mg+3 mg# per 3 ml] 3 ml 6 times per day](https://image.slidesharecdn.com/bronchodilator2-200831125338/85/Bronchodilators-16-320.jpg)


















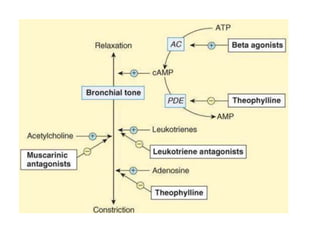
Bronchodilators are drugs used to relieve bronchospasms associated with respiratory disorders. The main classes of bronchodilators include adrenoceptor agonists like selective beta2 agonists, antimuscarinic bronchodilators, xanthine derivatives, and leukotriene antagonists. Beta2 agonists work by stimulating beta2 receptors in the lungs to promote bronchodilation. Antimuscarinics block acetylcholine's bronchoconstrictive effects. Xanthines like theophylline inhibit phosphodiesterase to increase cAMP and cause bronchodilation. Leukotriene receptor antagonists suppress the bronchoconstrictive effects of leukotrienes. Corticosteroids























































































