





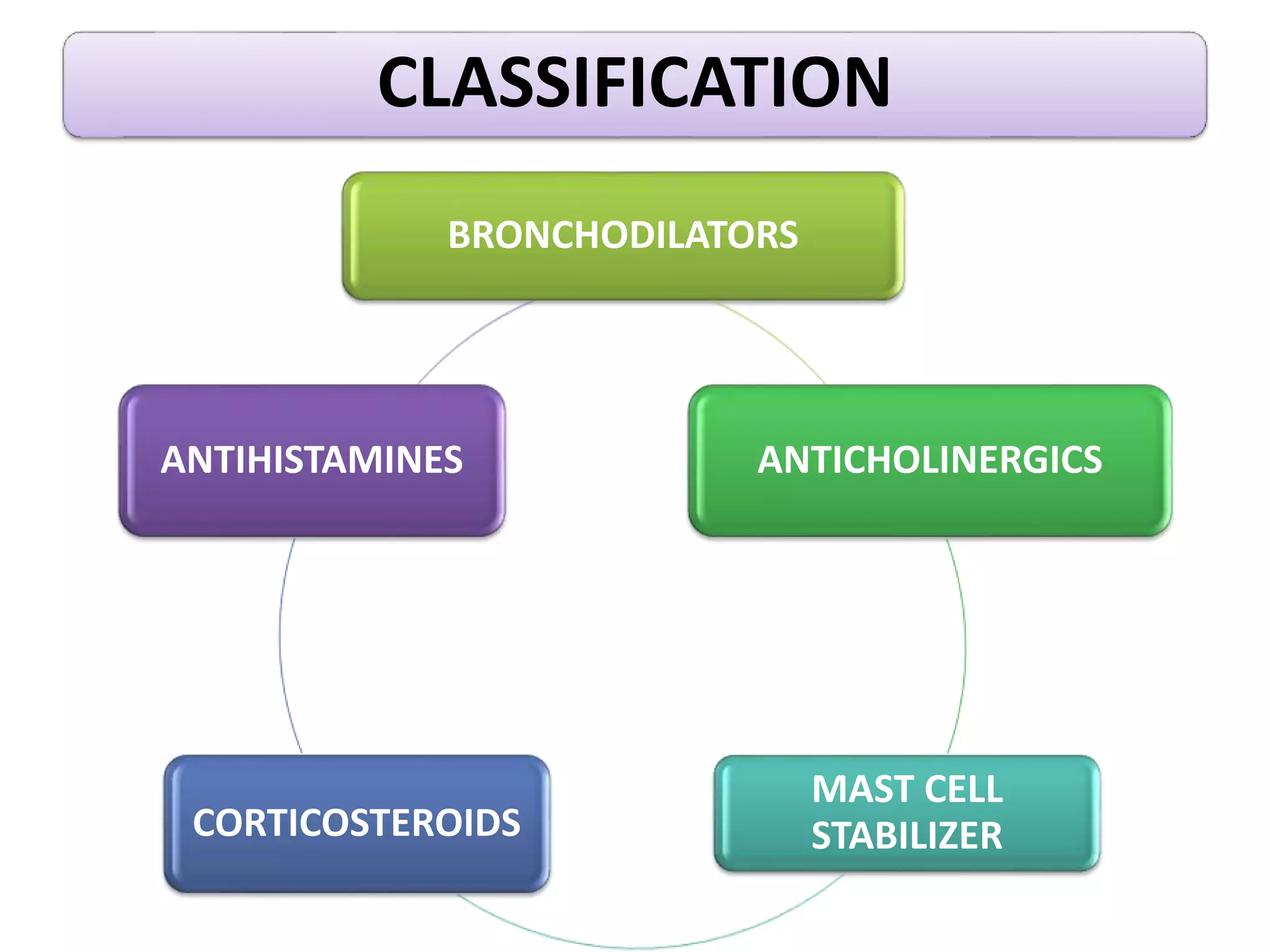






















This document discusses drugs for treating asthma, including bronchodilators, corticosteroids, mast cell stabilizers, and antihistamines. It covers the classification, mechanisms of action, examples, dosages, side effects and nursing responsibilities for these drug classes. Bronchodilators such as albuterol and terbutaline work by relaxing smooth muscles to open airways. Corticosteroids reduce inflammation and potentiate bronchodilators. Mast cell stabilizers inhibit mast cell activity to prevent mediator release. Antihistamines block the effects of histamine to relieve allergic reactions. The document also addresses treating status asthmaticus and drug interactions.























































































