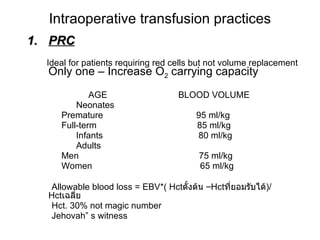
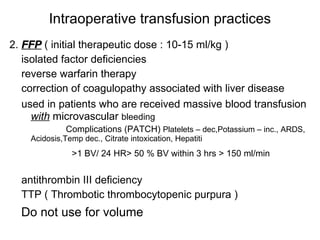
Blood transfusion practices involve determining a patient's blood type and screening for antibodies to reduce risks of transfusion reactions like hemolytic reactions. Key indications for transfusion include maintaining hemoglobin above 6-8 g/dL and allowing blood loss within established volumes. Complications can be minimized through proper blood type matching, leukoreduction, and following guidelines for transfusion thresholds and volumes.
























































![Blood Transfusions ED Powerpoint 12-03-13[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bloodtransfusionsedpowerpoint12-03-131-250306225306-4d317c5e-thumbnail.jpg?width=640&height=640&fit=bounds)
































