Downloaded 784 times


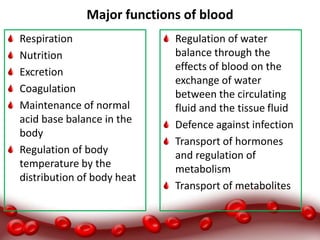
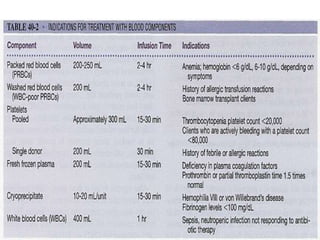

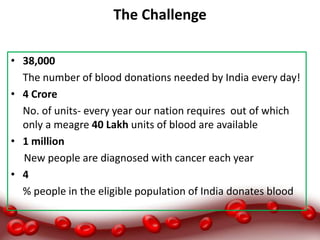
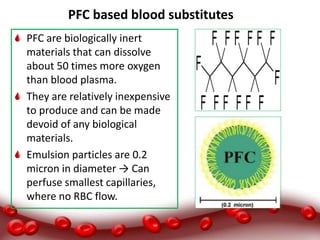




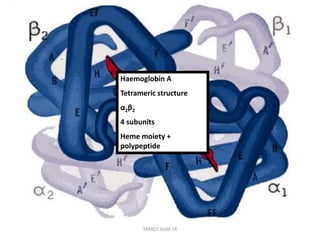

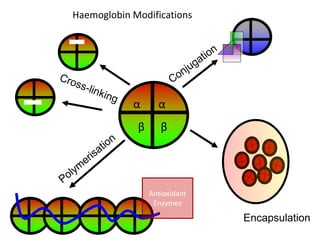
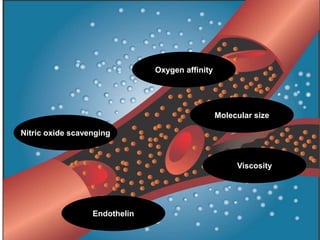
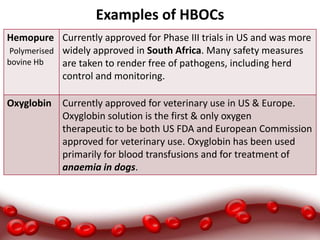



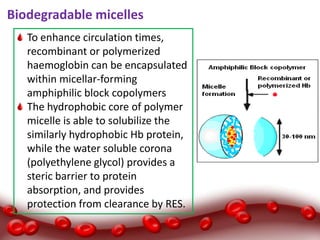



This document discusses blood substitutes and their development. It covers: - The functions of blood and the challenges in meeting demand for blood transfusions. - The types of blood substitutes including plasma expanders and red blood cell substitutes like hemoglobin-based oxygen carriers. - The ideal properties of blood substitutes and examples of products in development or approved, including challenges faced. - Perfluorocarbon-based products and hemoglobin-based products, discussing sources, modifications made and examples of some products.









































































