Downloaded 78 times
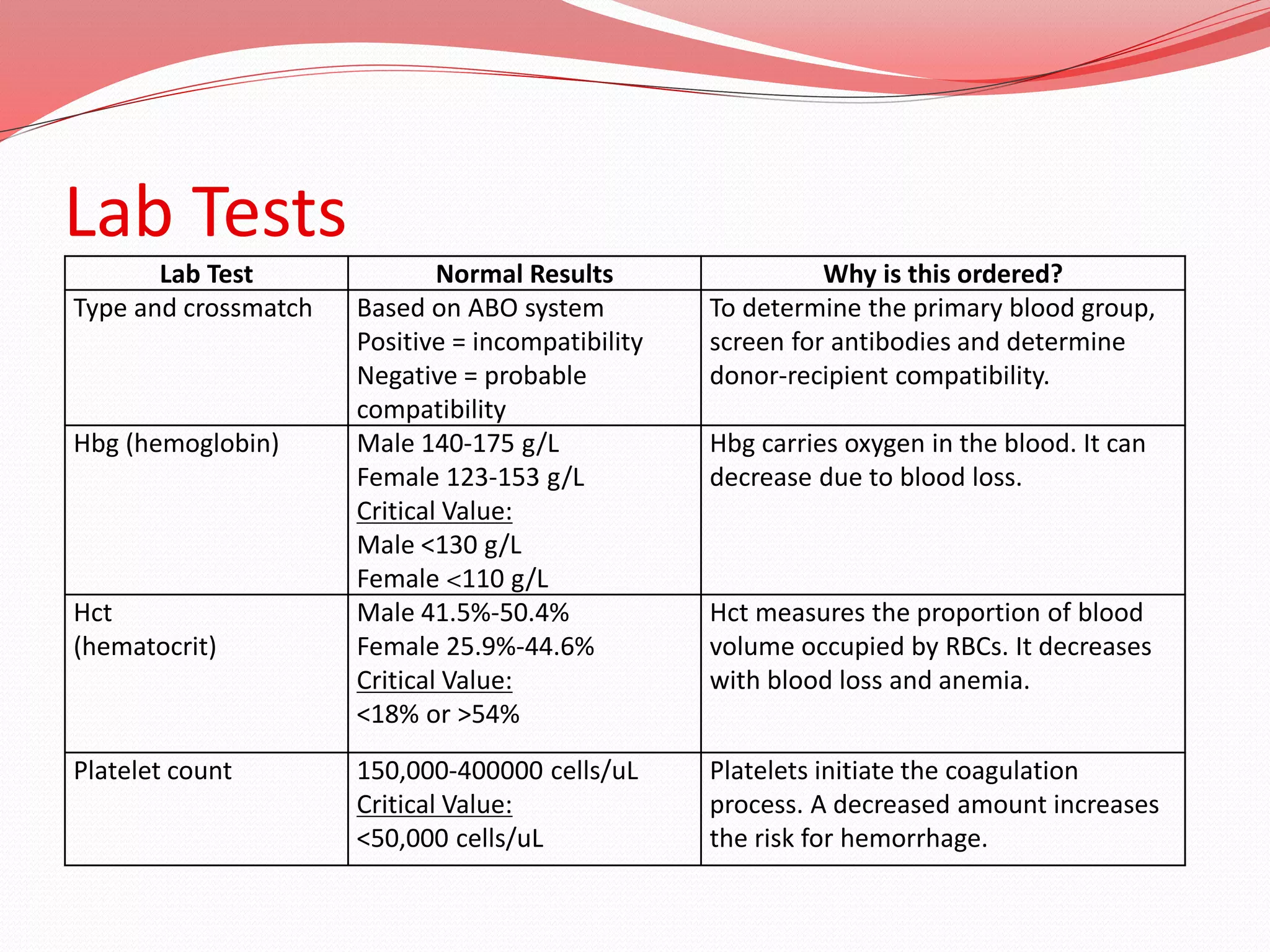
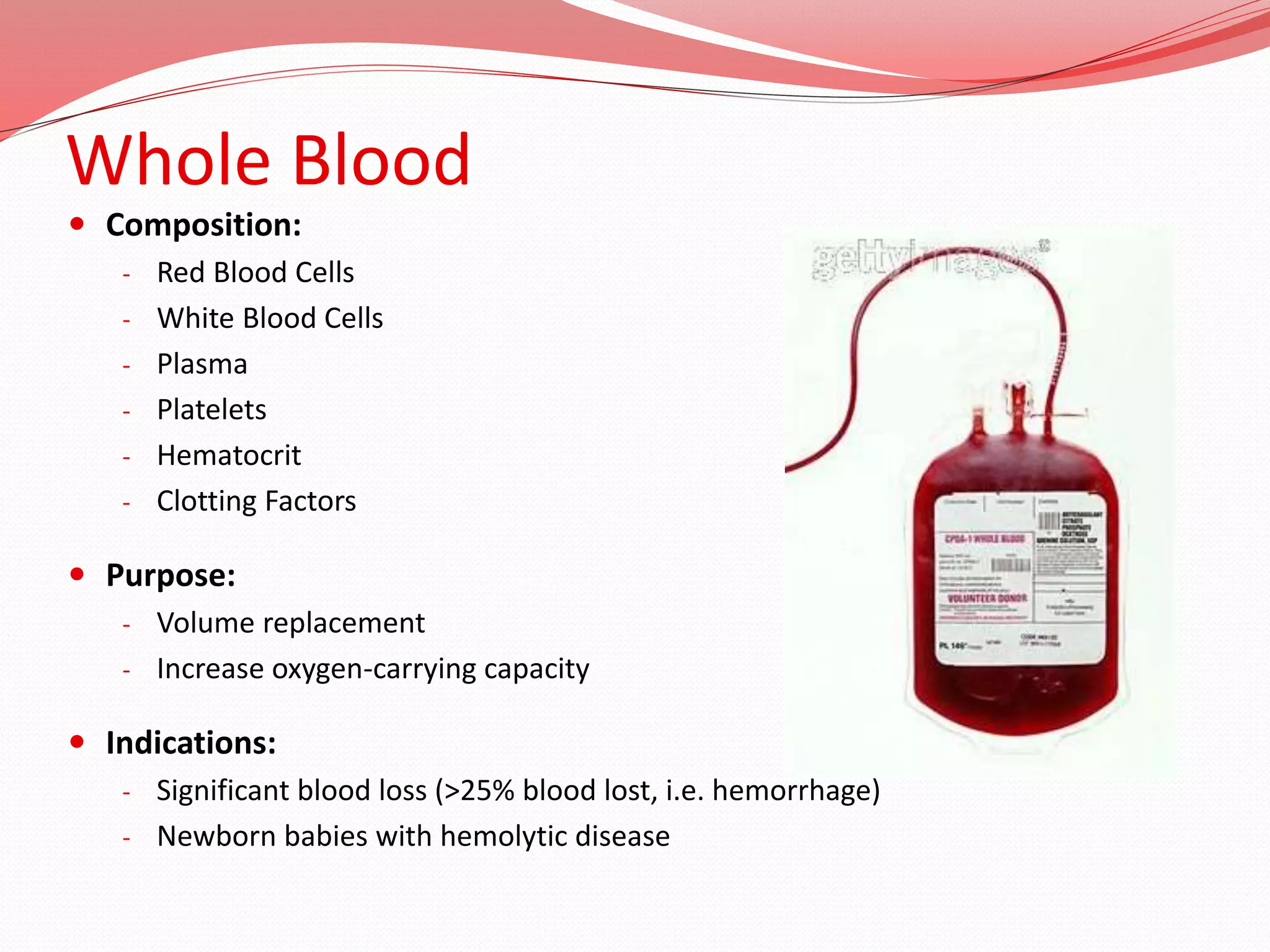
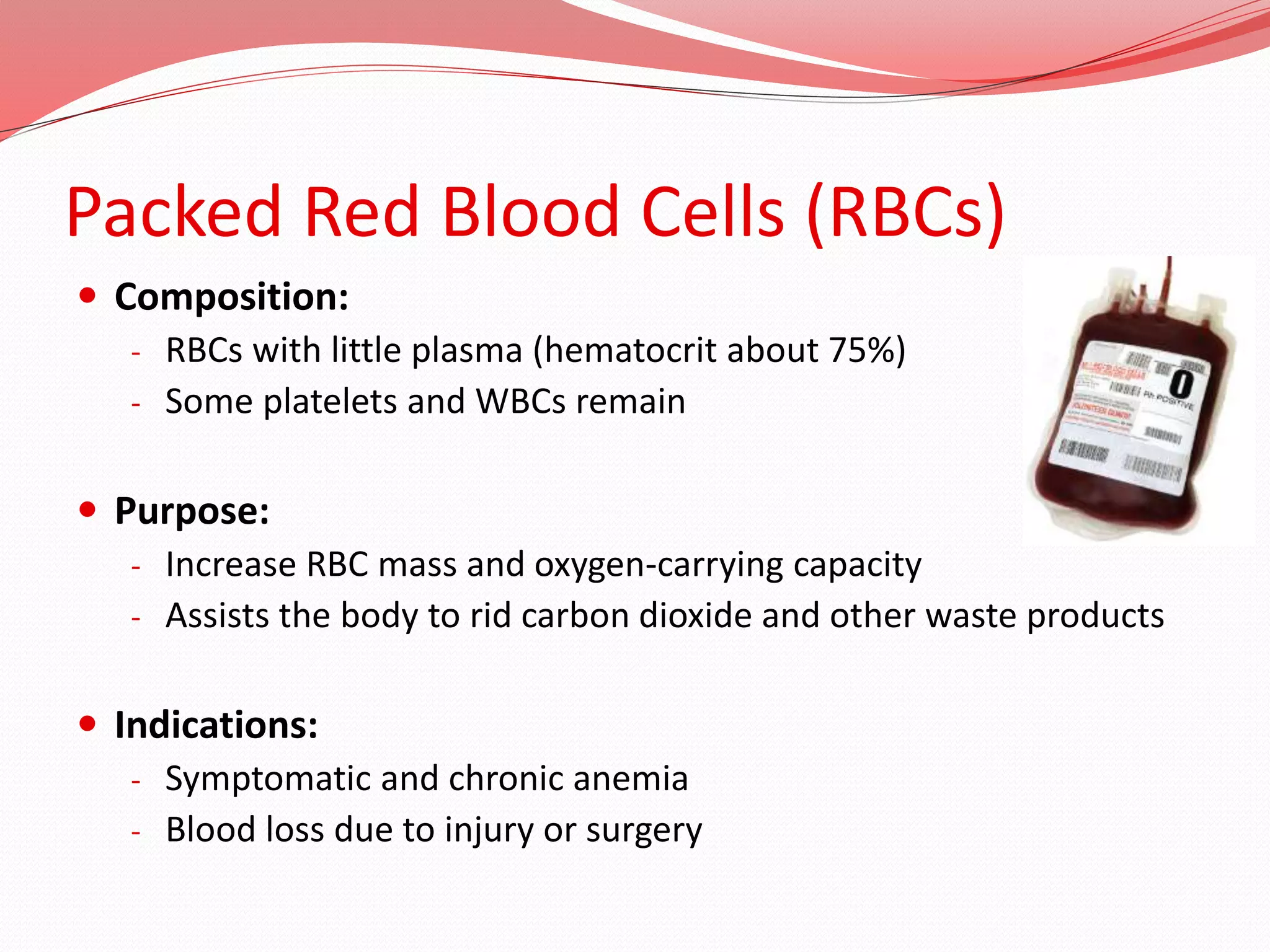
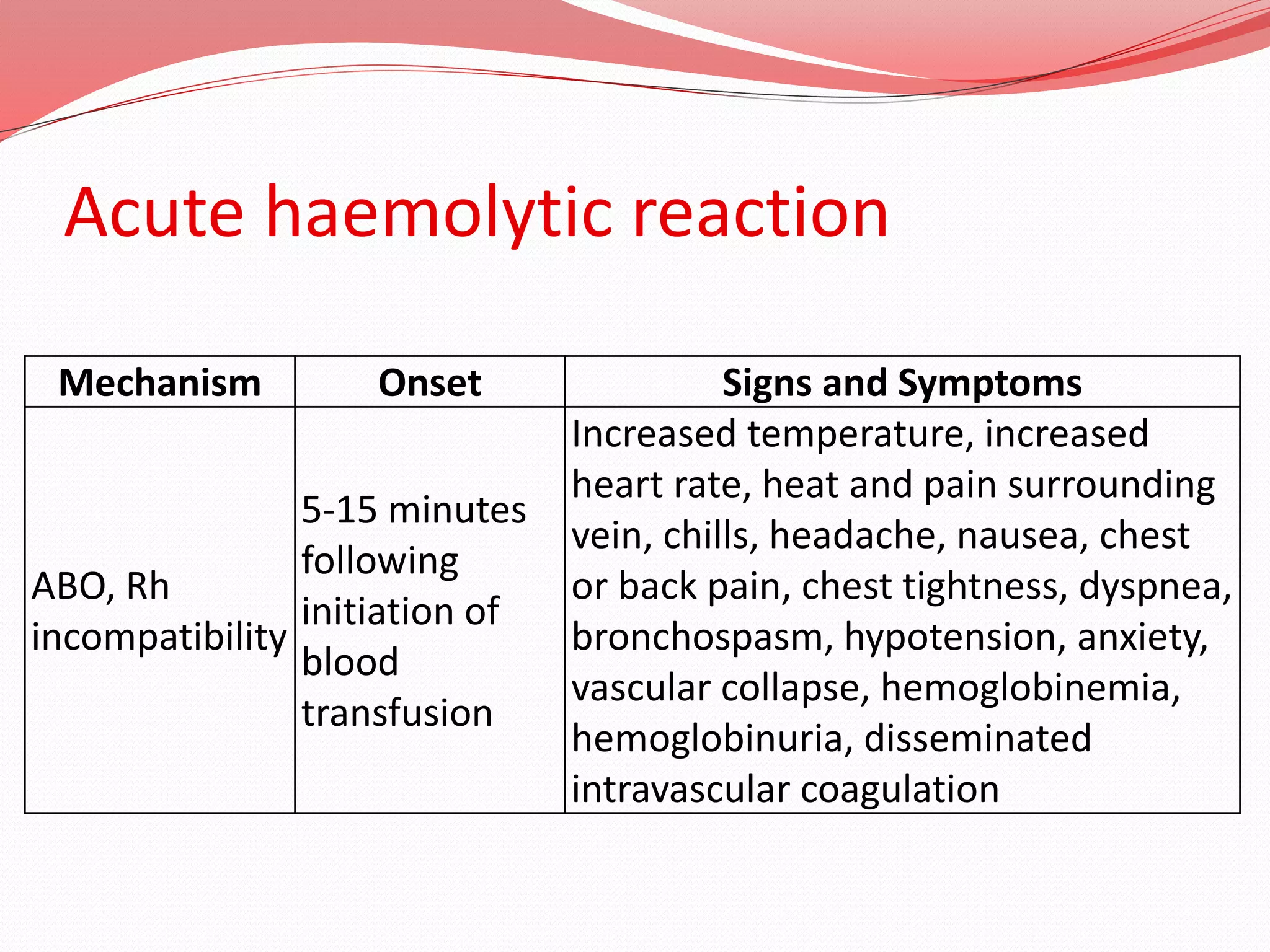
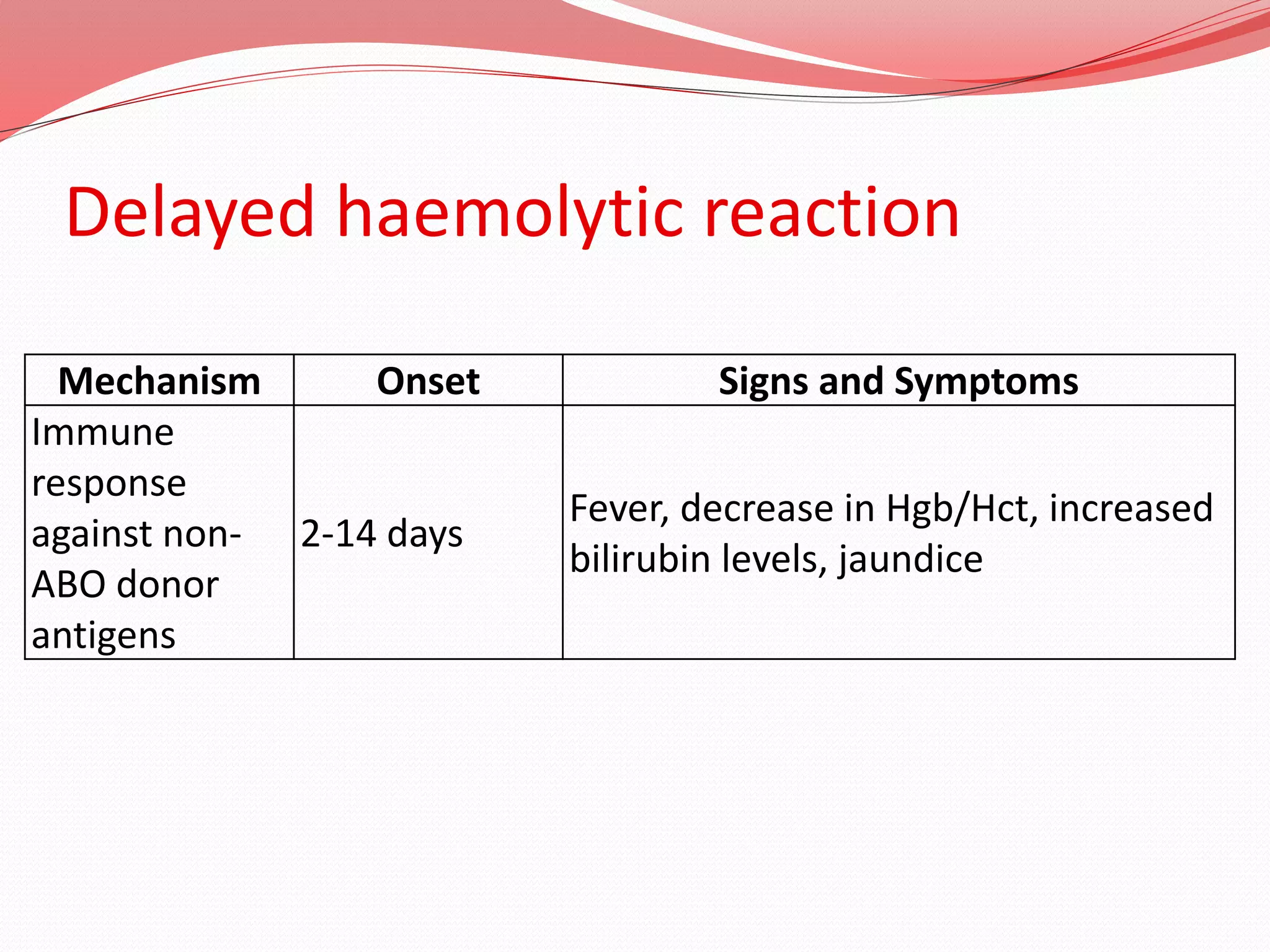
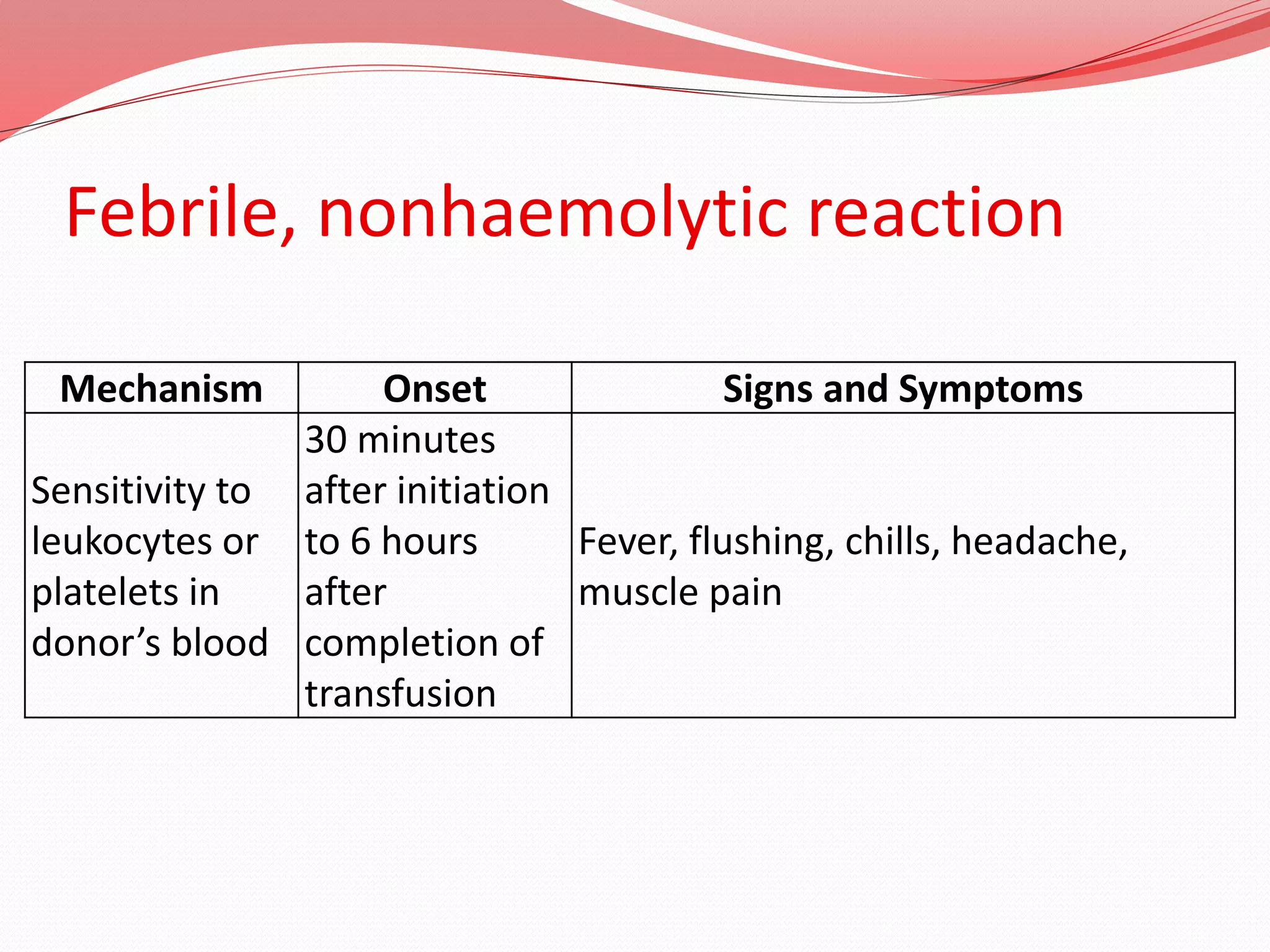
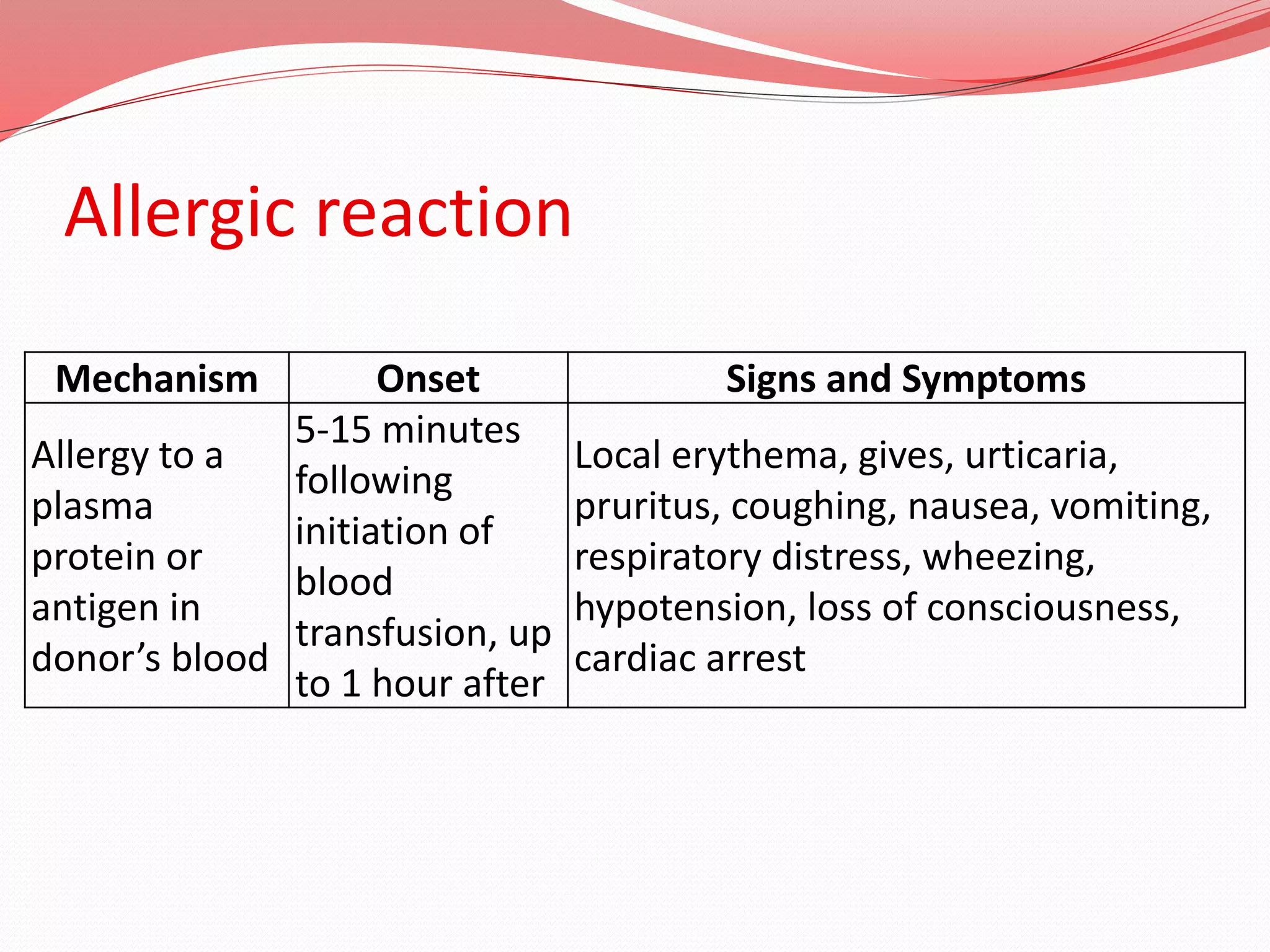
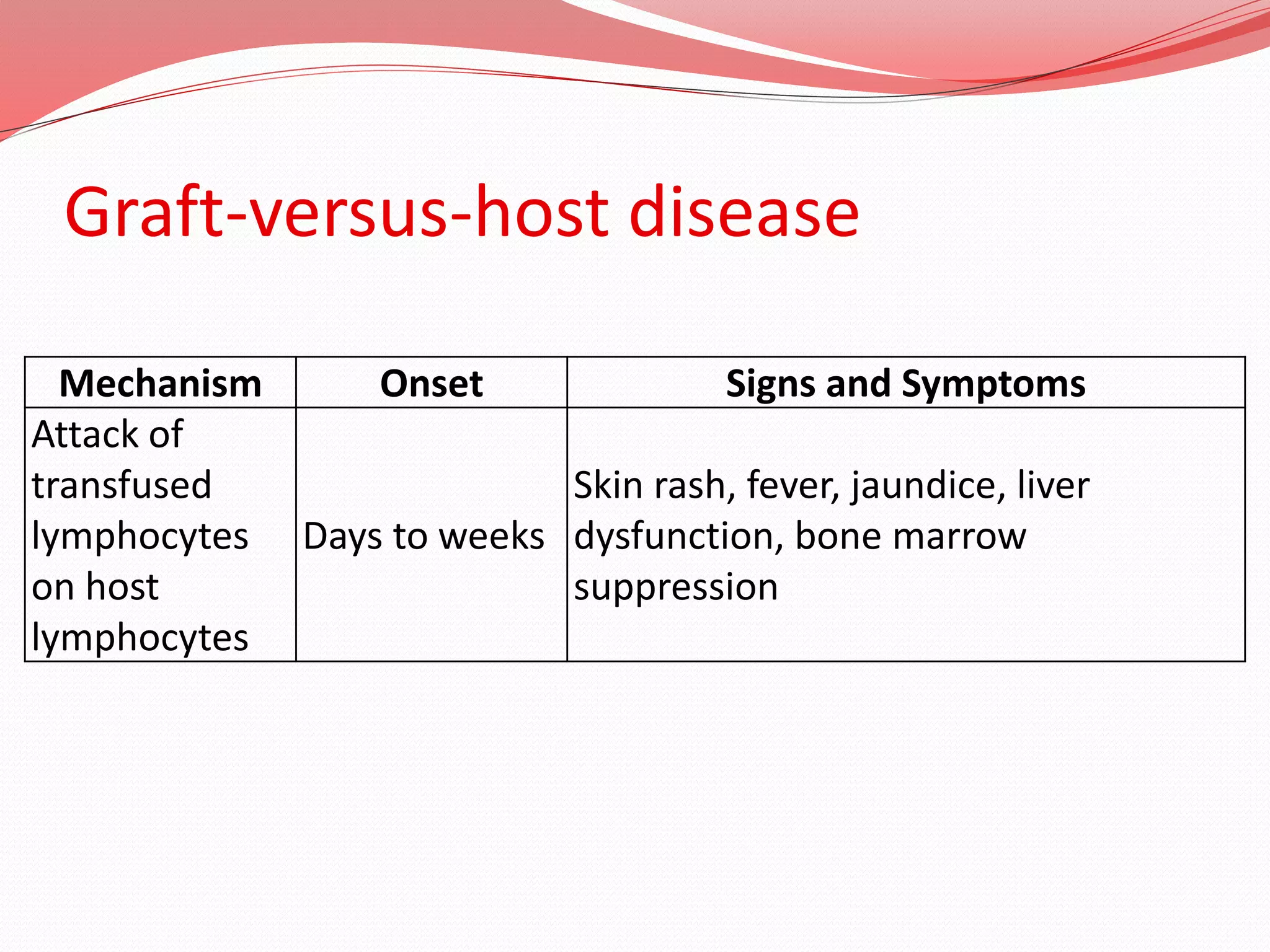
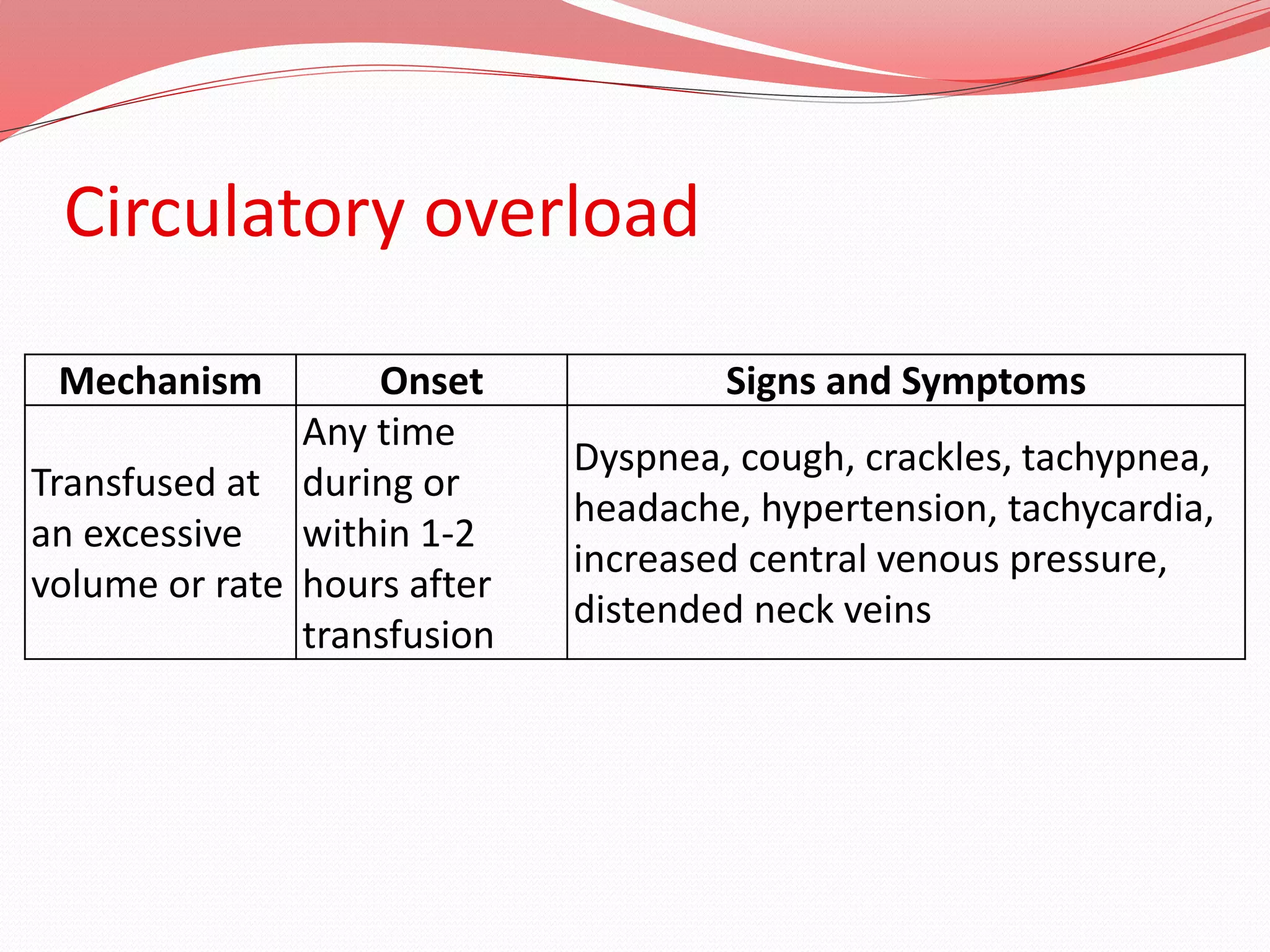
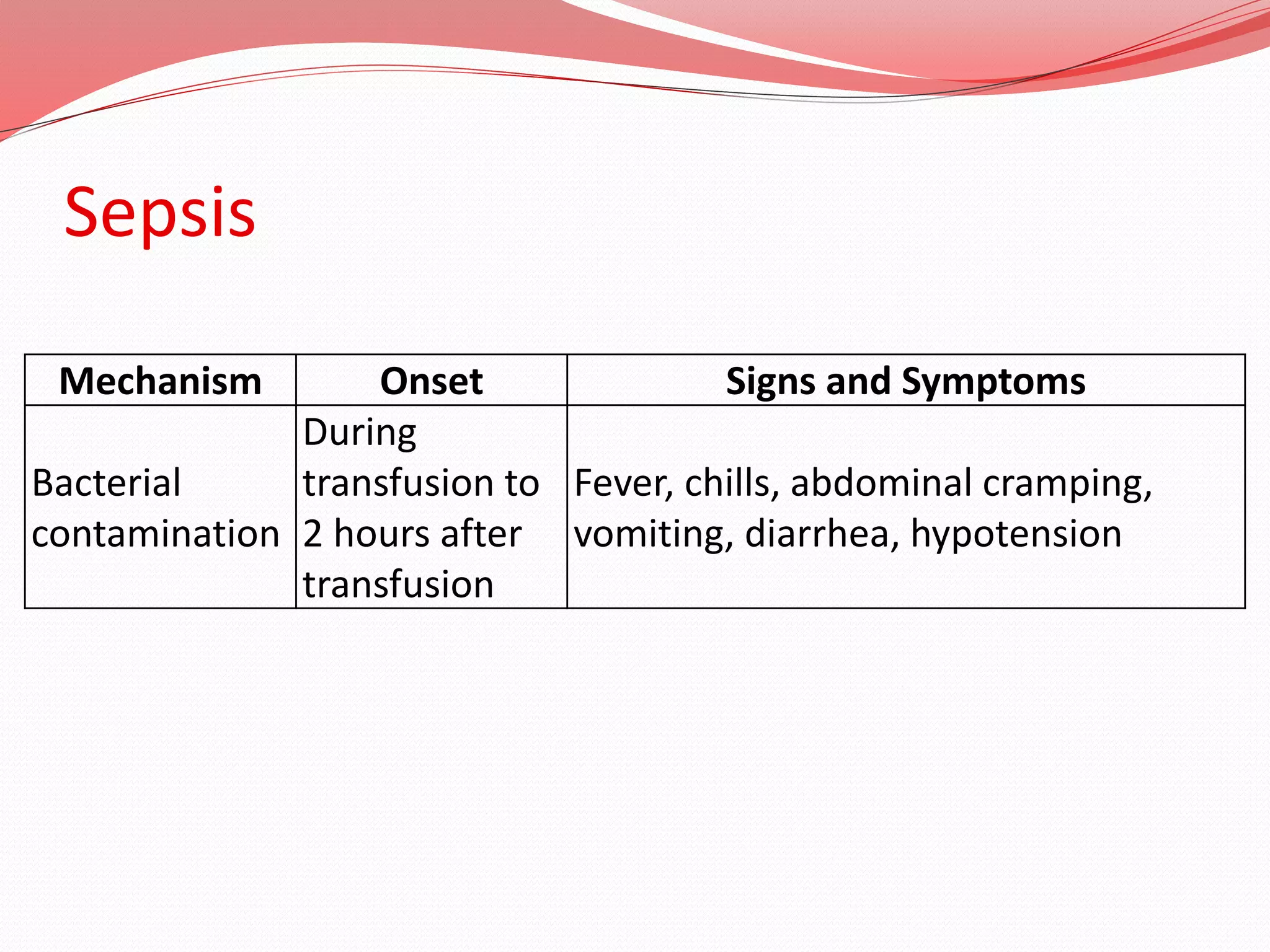
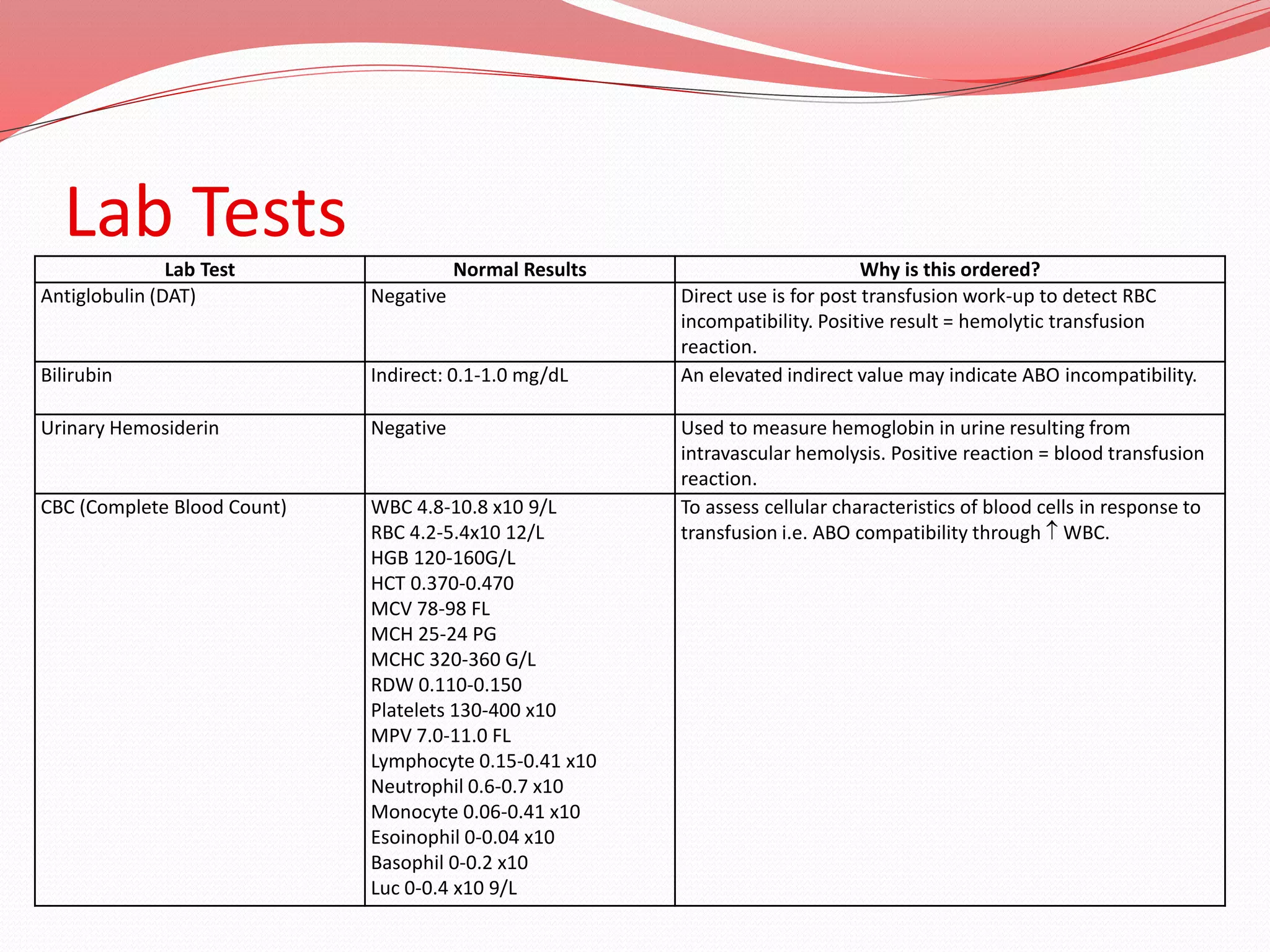
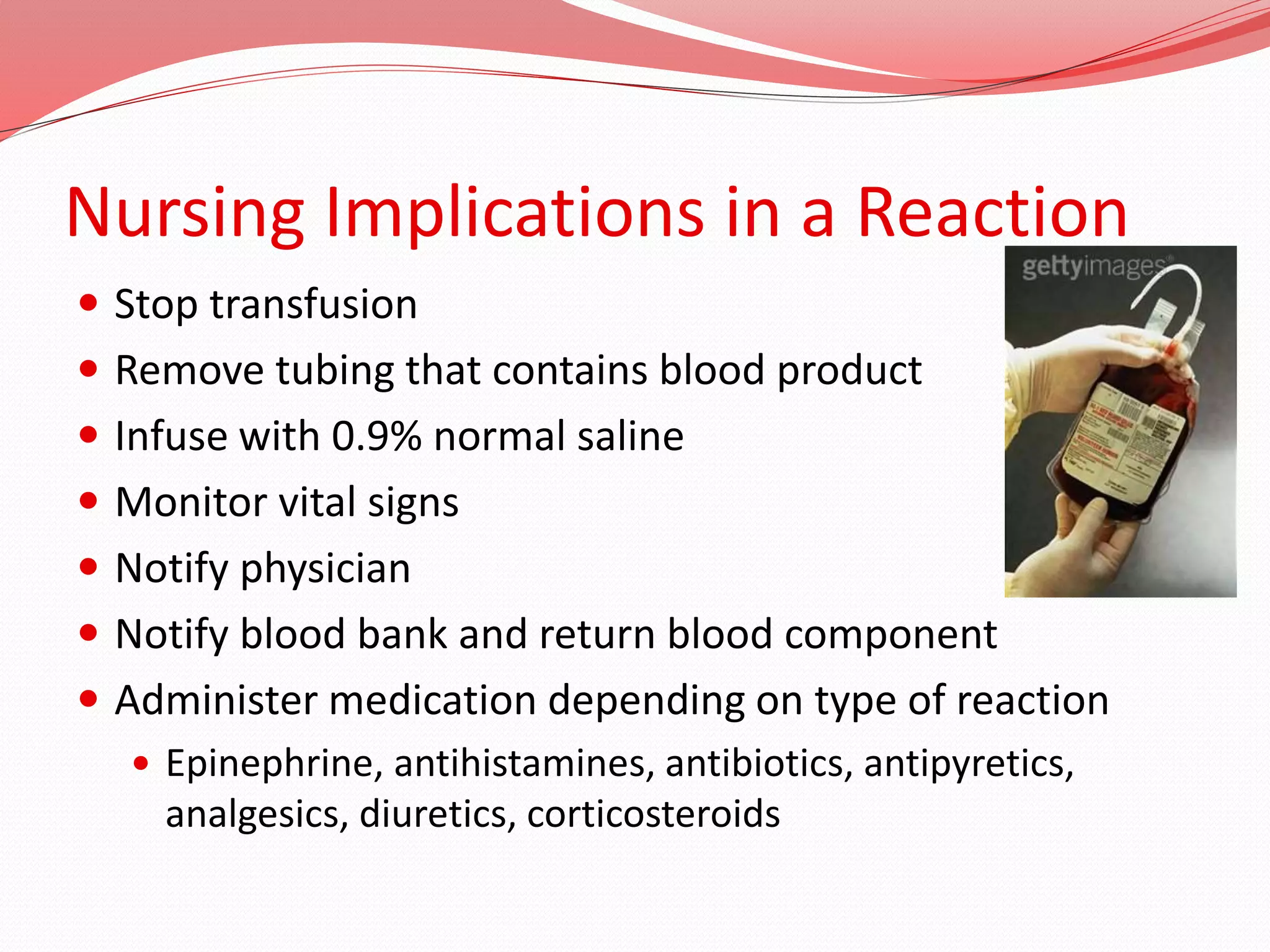


A blood transfusion is the administration of blood or blood components into a patient's circulatory system through an intravenous line. The main purposes are to restore blood volume, replace clotting factors, improve oxygen carrying capacity, and restore depleted blood elements. Indications for transfusion include significant blood loss, anemia, low platelet count, and coagulation disorders. Whole blood contains red blood cells, white blood cells, plasma, and platelets. Other blood products administered include packed red blood cells, platelets, fresh frozen plasma, and albumin. Nurses monitor patients during and after transfusion for signs of reactions and ensure documentation of the procedure.






































![Blood Transfusions ED Powerpoint 12-03-13[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bloodtransfusionsedpowerpoint12-03-131-250306225306-4d317c5e-thumbnail.jpg?width=640&height=640&fit=bounds)





































