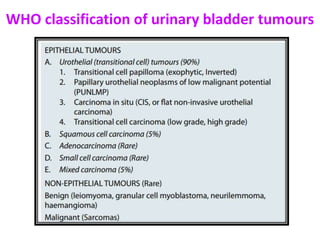

This document discusses various congenital anomalies, inflammations, and tumors of the lower urinary tract. It begins by describing common congenital anomalies like vesicoureteric reflux and double ureters. It then covers inflammations of the ureter, bladder, and urethra. The majority of the document discusses tumors of the bladder, including classification of urothelial/transitional cell tumors and their histological features. Non-epithelial bladder tumors and tumors of the renal pelvis and ureters are also briefly covered.























































































