Downloaded 423 times

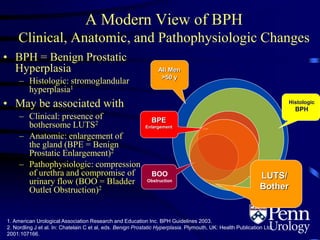
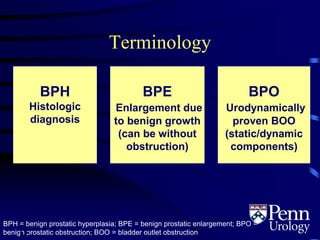
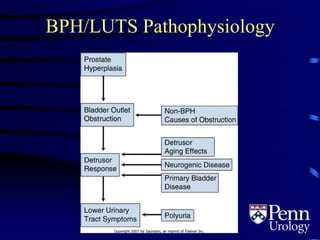
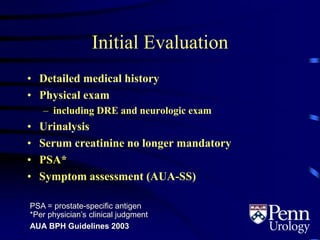
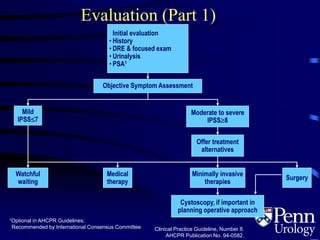
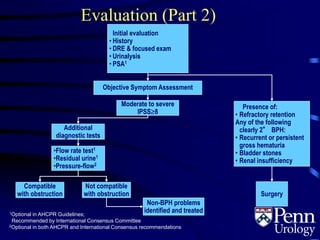





This document provides an overview of benign prostatic hyperplasia (BPH), including its epidemiology, terminology, evaluation, medical and surgical treatment options, and pathophysiology. Some key points include: - BPH is a histological diagnosis defined as nonmalignant hyperplasia of the prostate gland. It often presents clinically as bothersome lower urinary tract symptoms and an enlarged prostate. - Evaluation involves medical history, physical exam including DRE, urinalysis, and symptom assessment. Additional tests like flow rate and residual urine may be used if symptoms are moderate to severe. - Medical therapy options are alpha-blockers which target the dynamic component of obstruction, and 5-alpha-re






















![Benign Prostatic Hyperplasia BPH [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/bphedmond-140716213908-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






































































