Downloaded 88 times

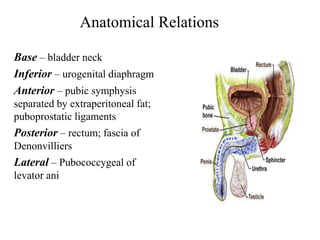

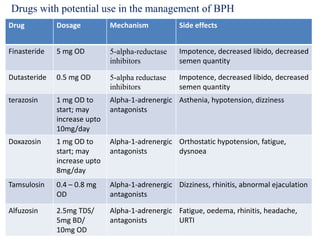


This document discusses benign prostatic hyperplasia (BPH) and its management. It begins by defining BPH as a benign enlargement of the prostate gland that commonly occurs in aging men. It then covers the anatomy and histology of the prostate, causes of BPH, pathophysiology and effects of BPH, symptoms, diagnostic tests including DRE, PSA, uroflowmetry, and management options like watchful waiting, lifestyle changes, medications such as alpha blockers and 5-ARIs, and surgeries.











































































