


















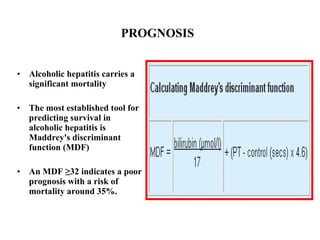












Alcoholic hepatitis is a common condition caused by heavy alcohol consumption that carries a high mortality risk. Key aspects include: - Presentation includes jaundice, fever, tender hepatomegaly and abnormal liver function tests. - Severity is assessed using Maddrey's discriminant function, with scores over 32 indicating poor prognosis. - Treatment of severe cases involves corticosteroids to reduce immune-mediated injury, pentoxifylline to inhibit tumor necrosis factor production, and nutritional support to address negative nitrogen balance and increased energy needs. - Corticosteroids and pentoxifylline have been shown to improve short-term survival in randomized controlled trials for patients with severe disease.
































































































