Downloaded 500 times
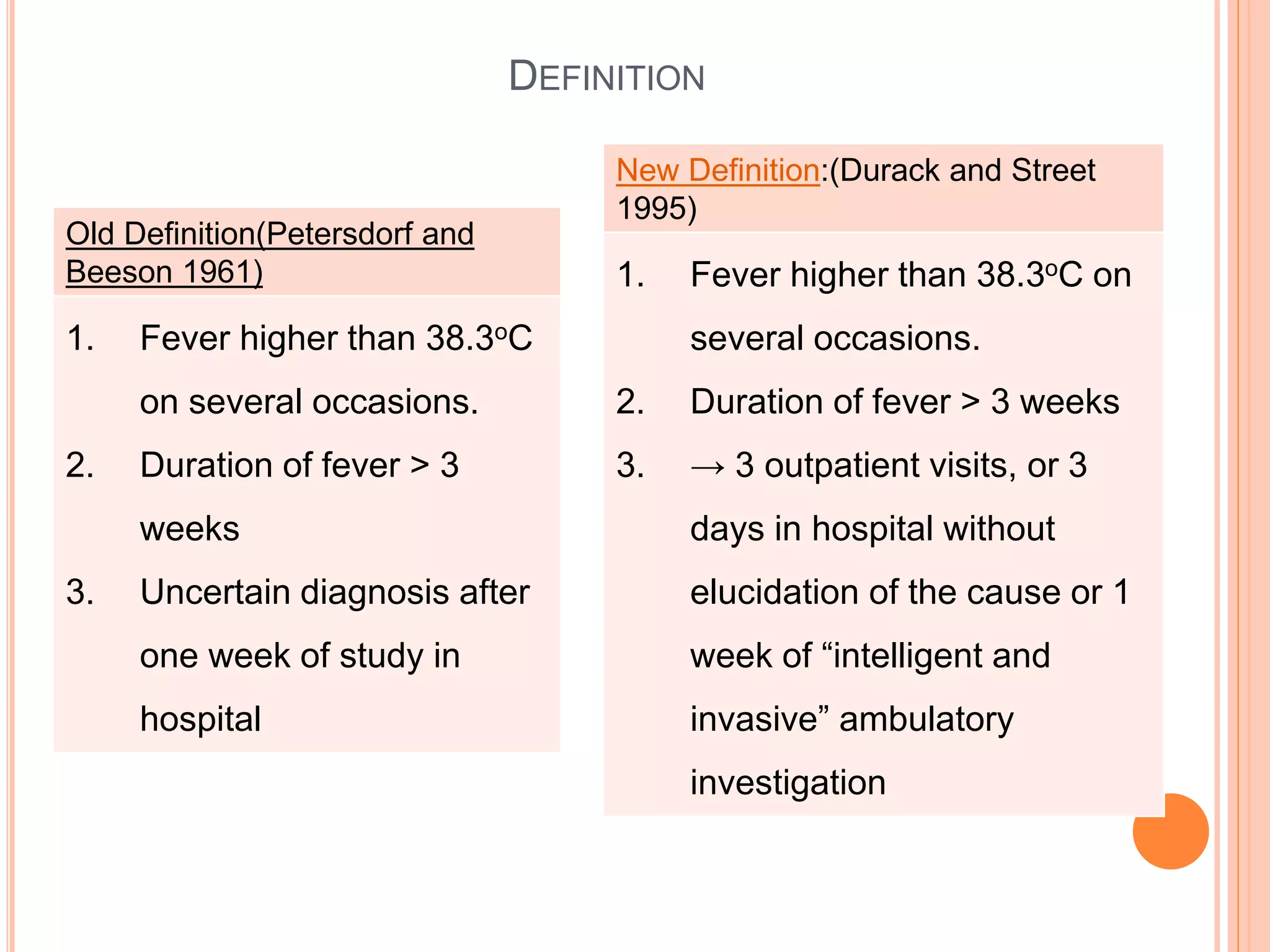
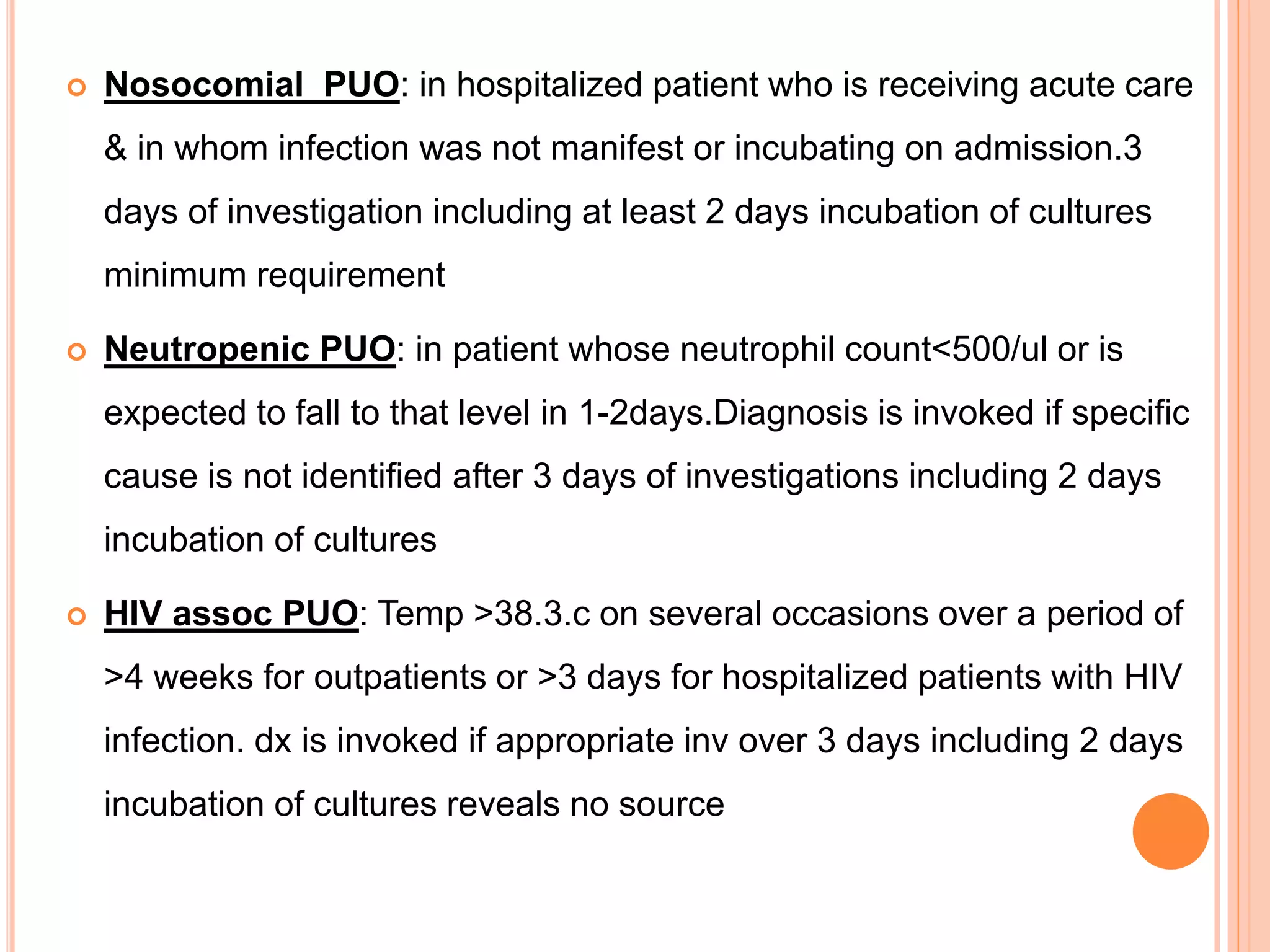
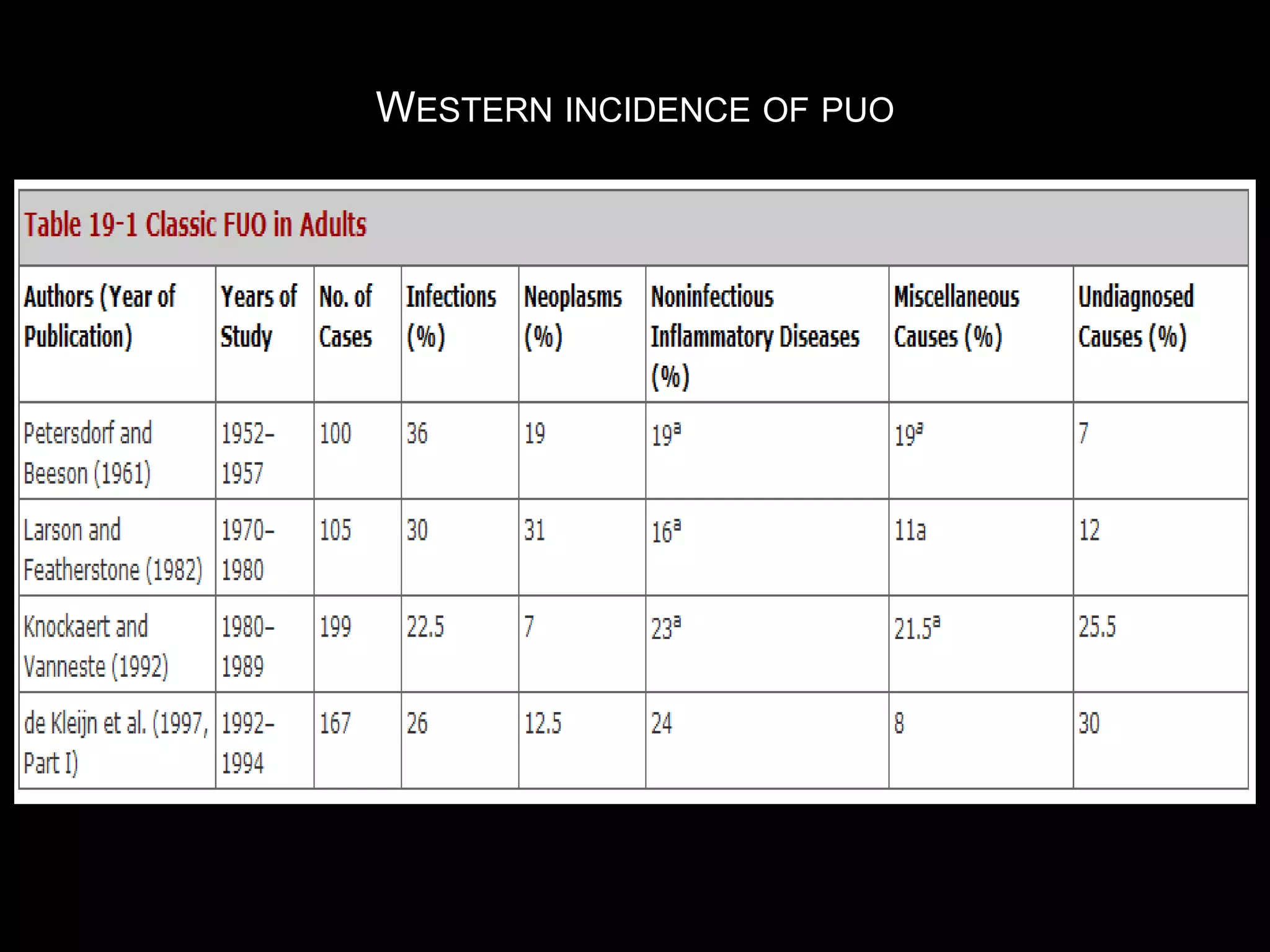
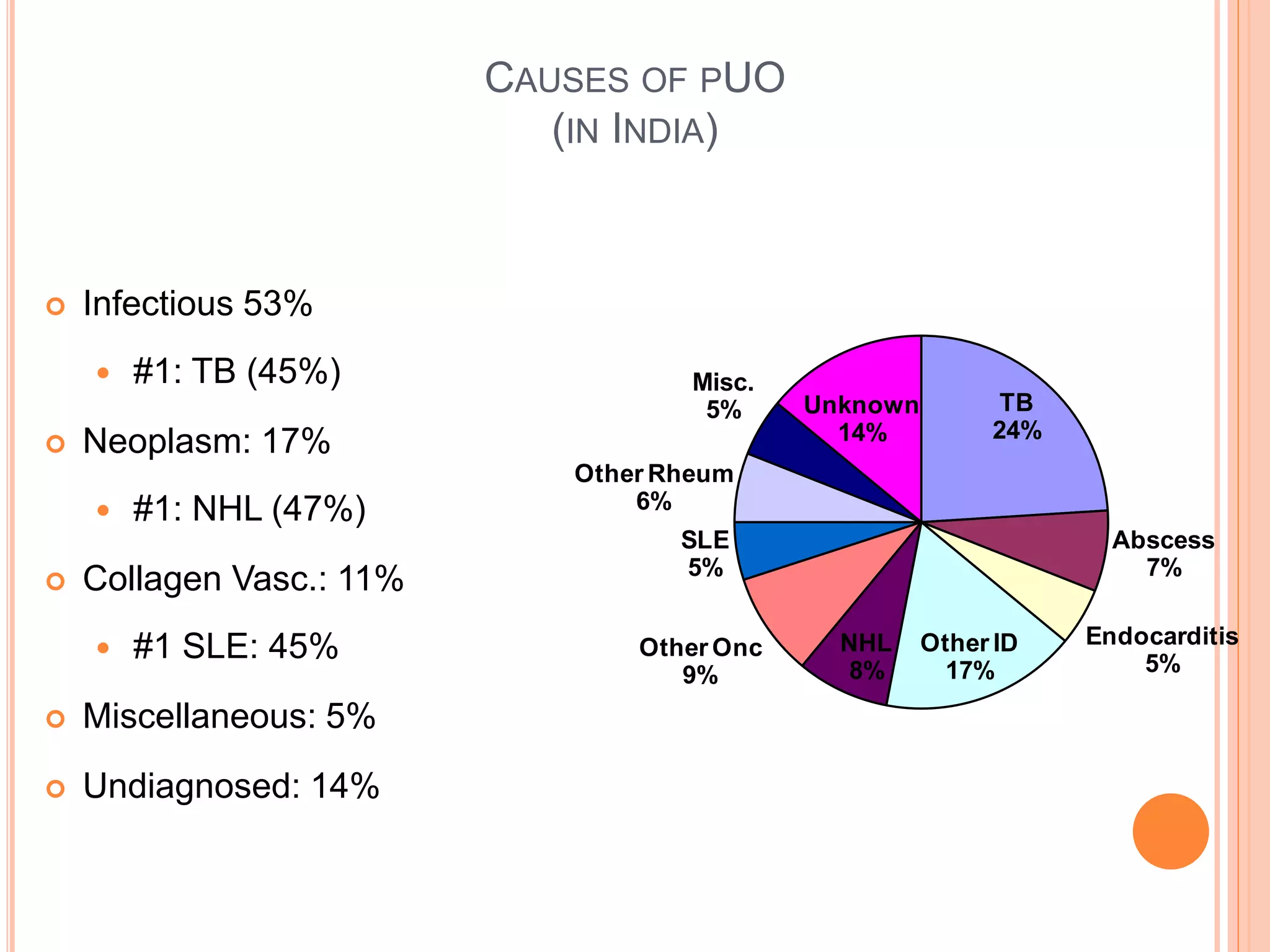
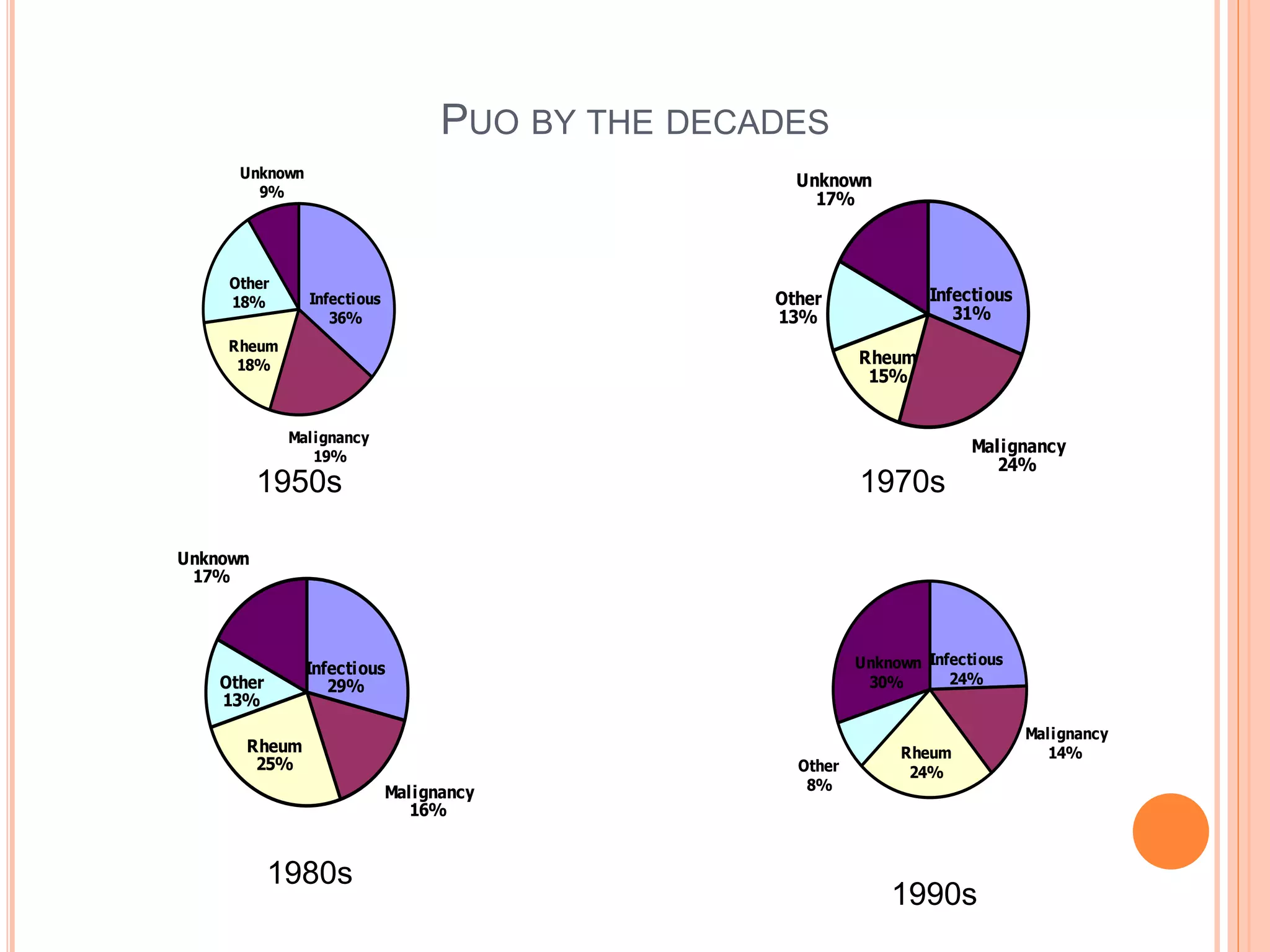



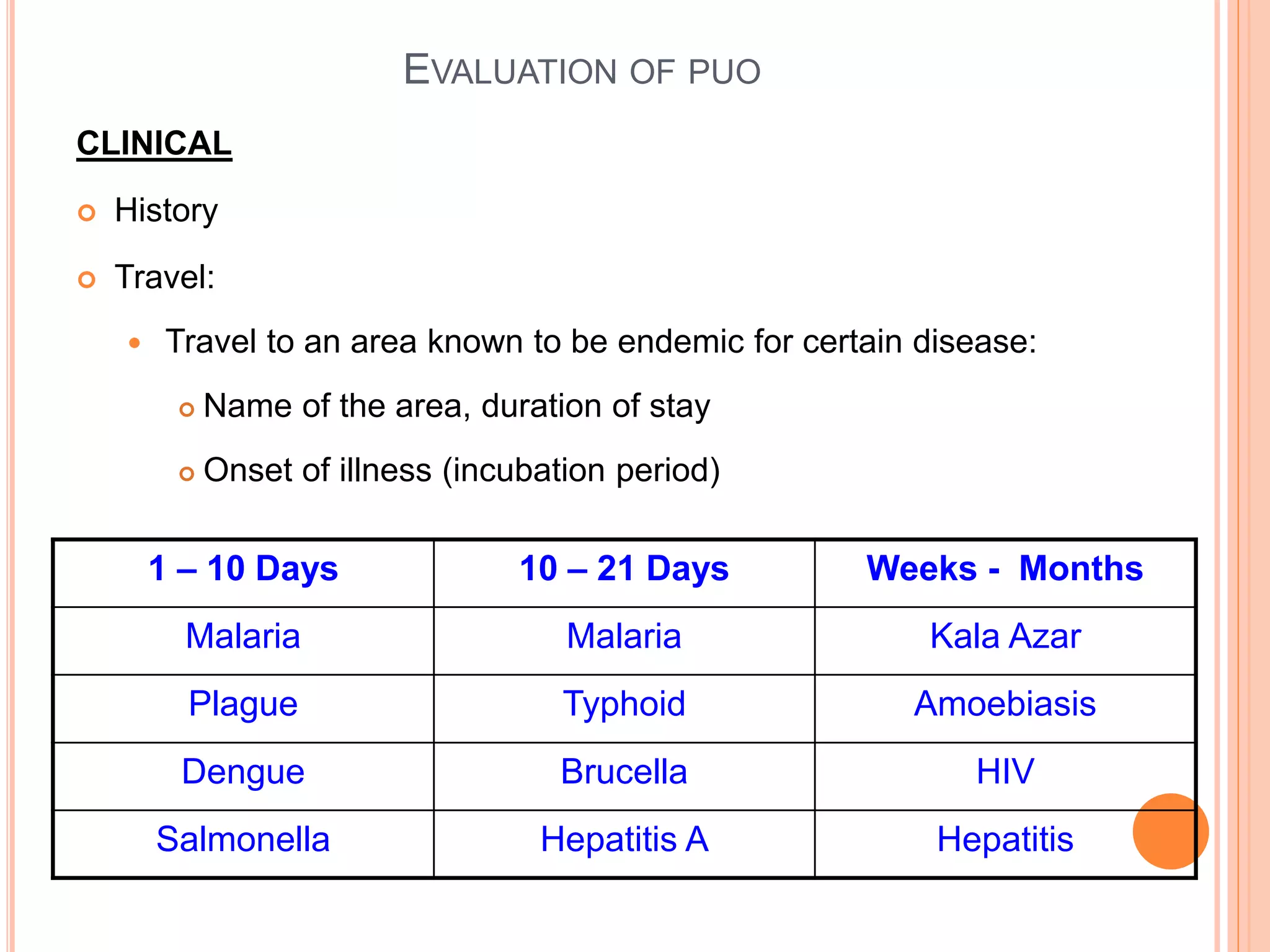
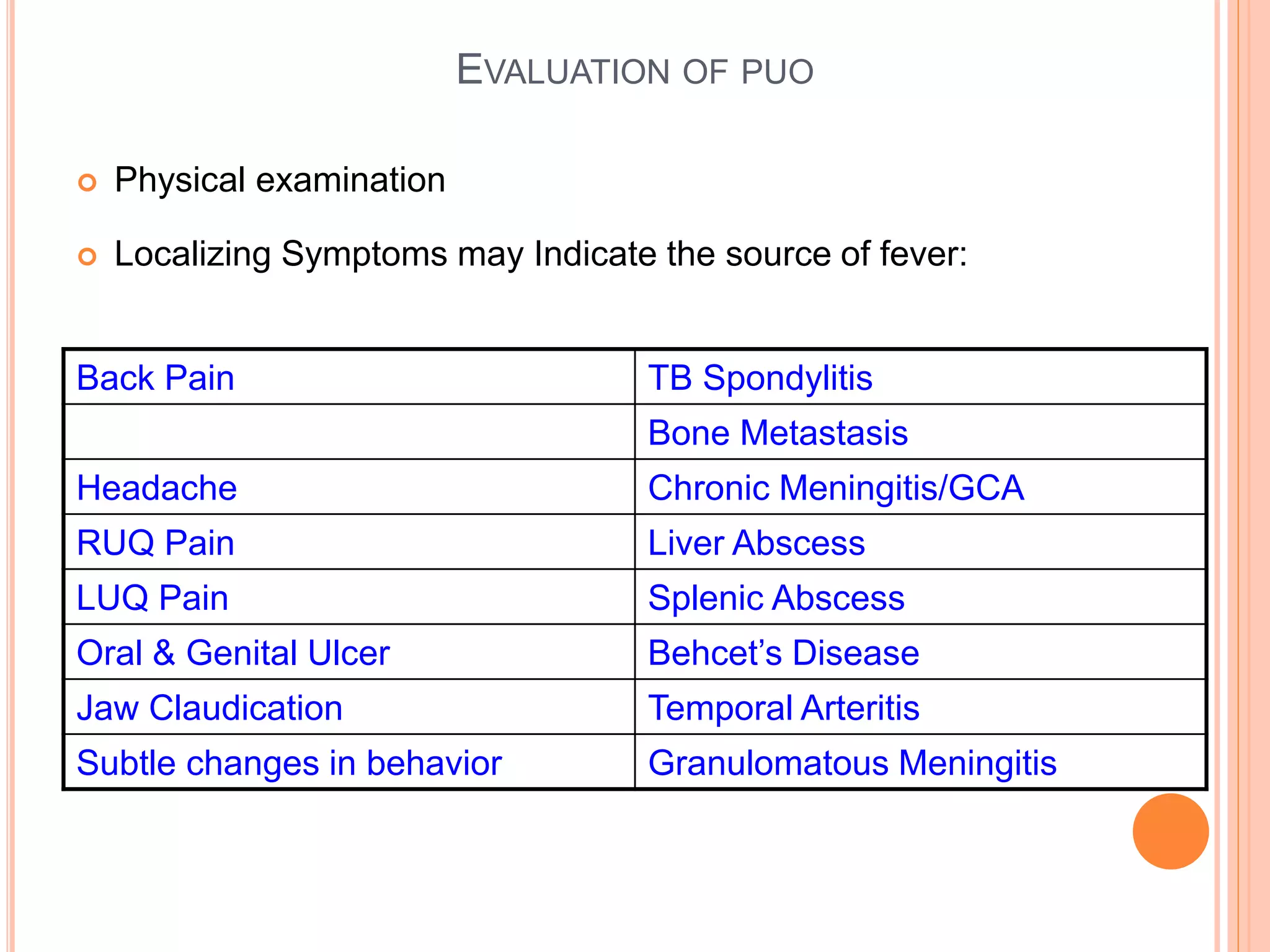
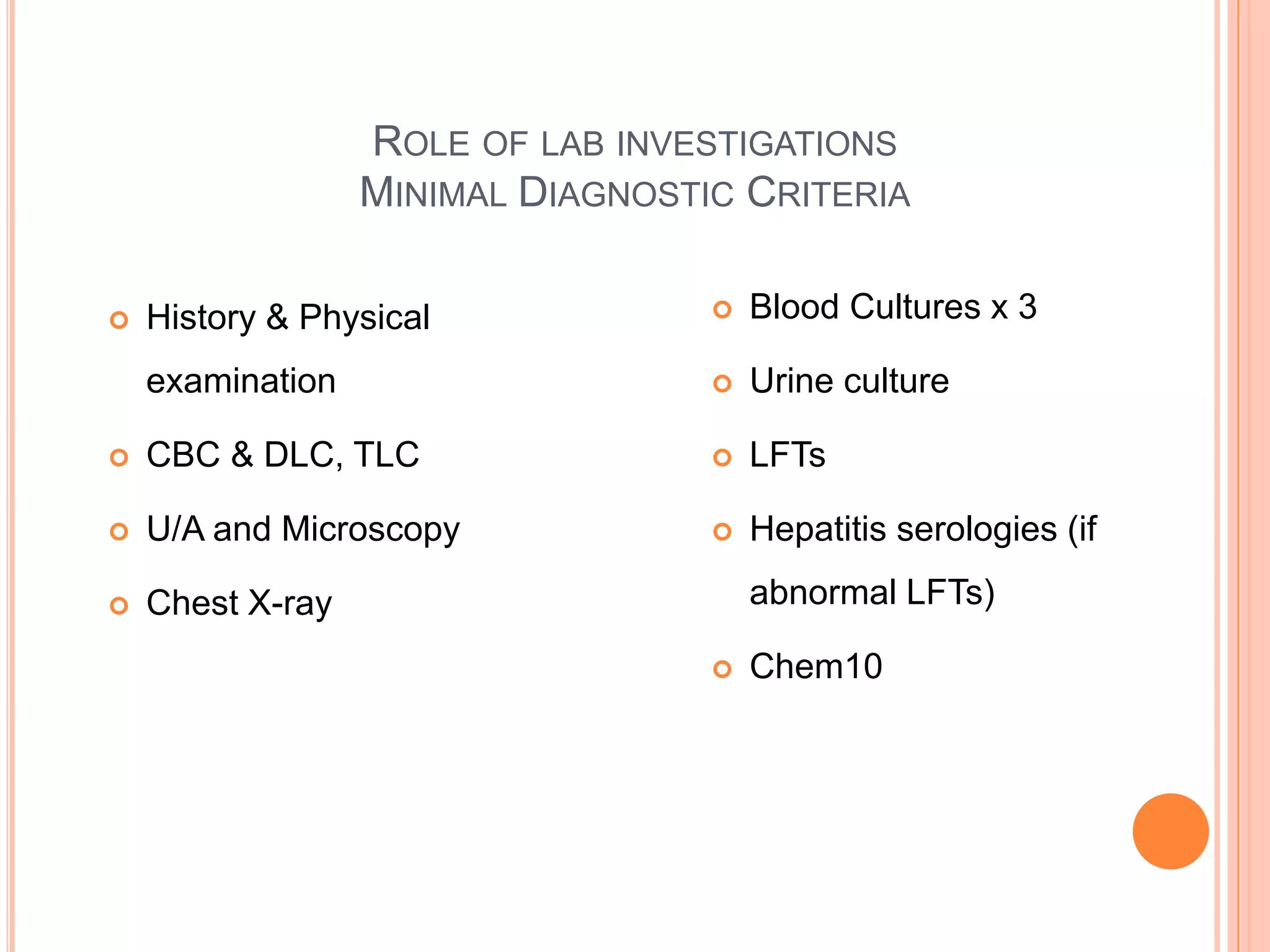
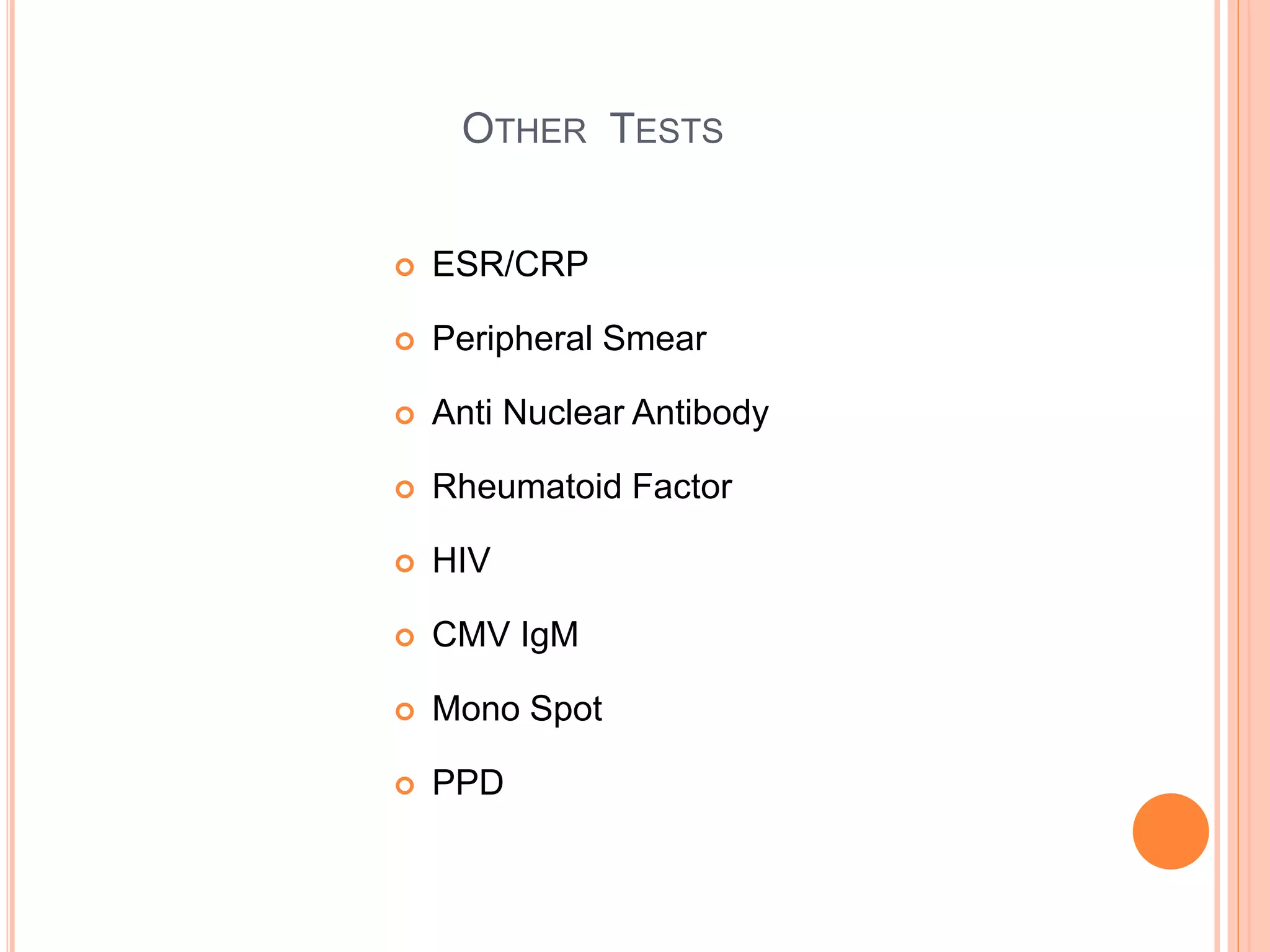
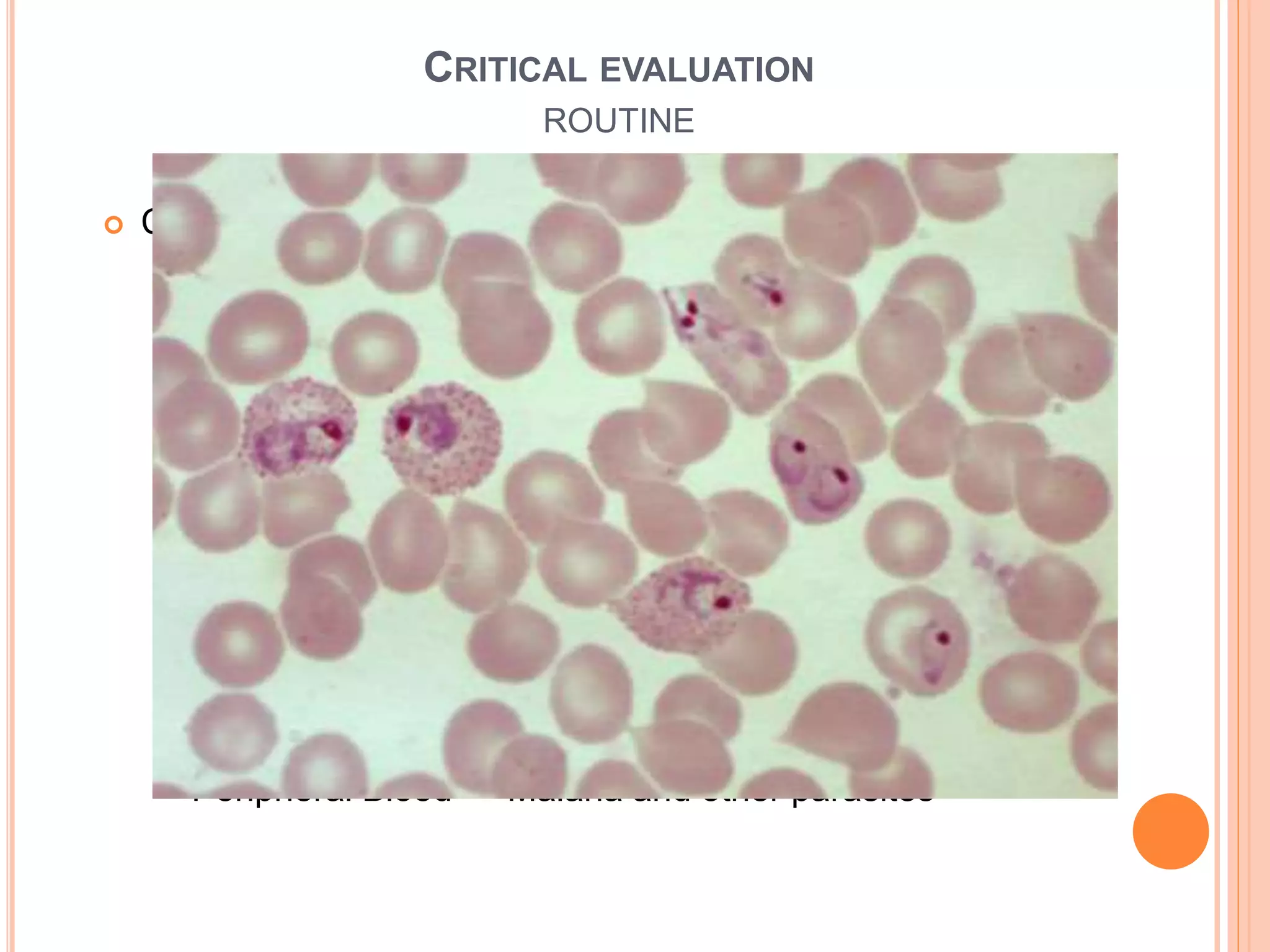

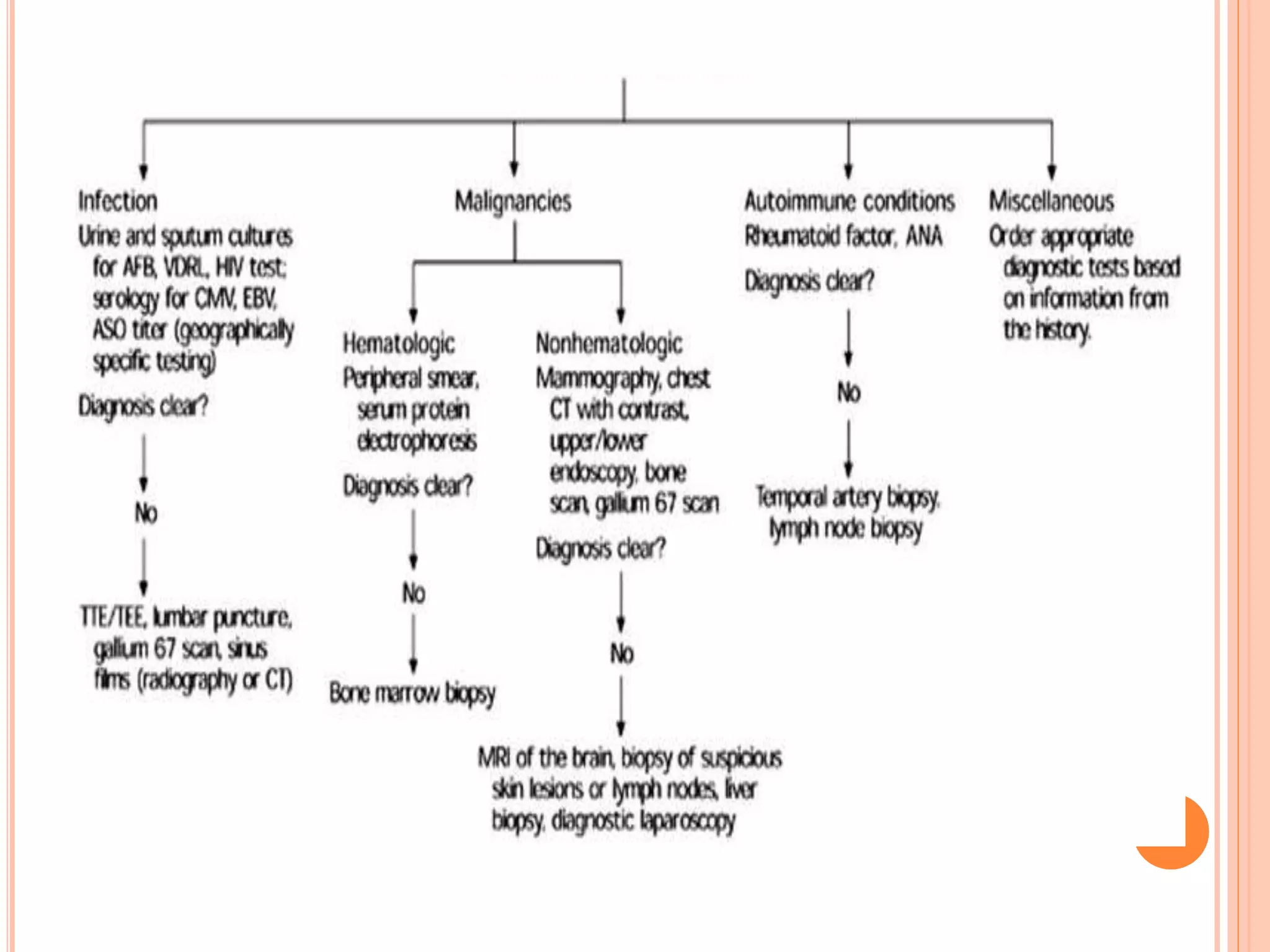


This document discusses pyrexia of unknown origin (PUO). It begins by defining PUO according to old and new definitions. It then expands the new definition to include categories like nosocomial PUO, neutropenic PUO, and HIV-associated PUO. The document goes on to discuss the causes of PUO in different regions and time periods, with infectious diseases like tuberculosis being very common. It also outlines the evaluation and diagnostic approach for PUO, including relevant laboratory tests, physical exam findings, and potential etiologies.























































































