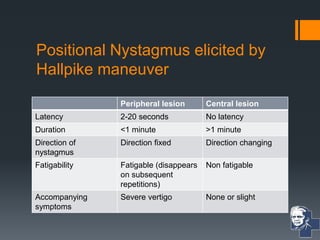
The document details various clinical and laboratory tests used to assess vestibular functions, including spontaneous nystagmus, Romberg's test, and caloric testing. It explains the distinctions between peripheral and central nystagmus as well as conditions that affect vestibular function. Additionally, it describes specific diagnostic maneuvers and tests for cerebellar and vestibular impairment.